The Clinical Outcomes of Transcatheter Microcoil Embolization in Patients with Active Lower Gastrointestinal Bleeding in the Small Bowel
- Affiliations
-
- 1Department of Radiology, Chonbuk National University Medical School and Hospital, Chonju 560-182, Korea. ymhan@chonbuk.ac.kr
- 2Research Institute of Clinical Medicine, Chonbuk National University Medical School and Hospital, Chonju 560-182, Korea.
- 3Institute of Cardiovascular Research, Chonbuk National University Medical School and Hospital, Chonju 560-182, Korea.
- 4Department of Internal Medicine, Chonbuk National University Medical School and Hospital, Chonju 560-182, Korea.
- KMID: 1777268
- DOI: http://doi.org/10.3348/kjr.2009.10.4.391
Abstract
OBJECTIVE
To assess the clinical outcomes of the transcatheter microcoil embolization in patients with active lower gastrointestinal (LGI) bleeding in the small bowel, as well as to compare the mortality rates between the two groups based on the visualization or non-visualization of the bleeding focus determined by an angiography.
MATERIALS AND METHODS
We retrospectively evaluated all of the consecutive patients who underwent an angiography for treatment of acute LGI bleeding between January 2003 and October 2007. In total, the study included 36 patients who underwent a colonoscopy and were diagnosed to have an active bleeding in the LGI tracts. Based on the visualization or non-visualization of the bleeding focus, determined by an angiography, the patients were classified into two groups. The clinical outcomes included technical success, clinical success (no rebleeding within 30 days), delayed rebleeding (> 30 days), as well as the major and minor complication rates.
RESULTS
Of the 36 patients, 17 had angiography-proven bleeding that was distal to the marginal artery. The remaining 19 patients did not have a bleeding focus based on the angiography results. The technical and clinical success rates of performing transcatheter microcoil embolizations in patients with active bleeding were 100% and 88%, respectively (15 of 17). One patient died from continued LGI bleeding and one patient received surgery to treat the continued bleeding. There was no note made on the delayed bleeding or on the major or minor complications. Of the 19 patients without active bleeding, 16 (84%) did not have recurrent bleeding. One patient died due to continuous bleeding and multi-organ failure.
CONCLUSION
The superselective microcoil embolization can help successfully treat patients with active LGI bleeding in the small bowel, identified by the results of an angiography. The mortality rate is not significantly different between the patients of the visualization and non-visualization groups on angiography.
MeSH Terms
Figure
-

Fig. 1 Treatment modalities for 36 patients with lower gastrointestinal hemorrhaging. Tx = treatment, pts = patients
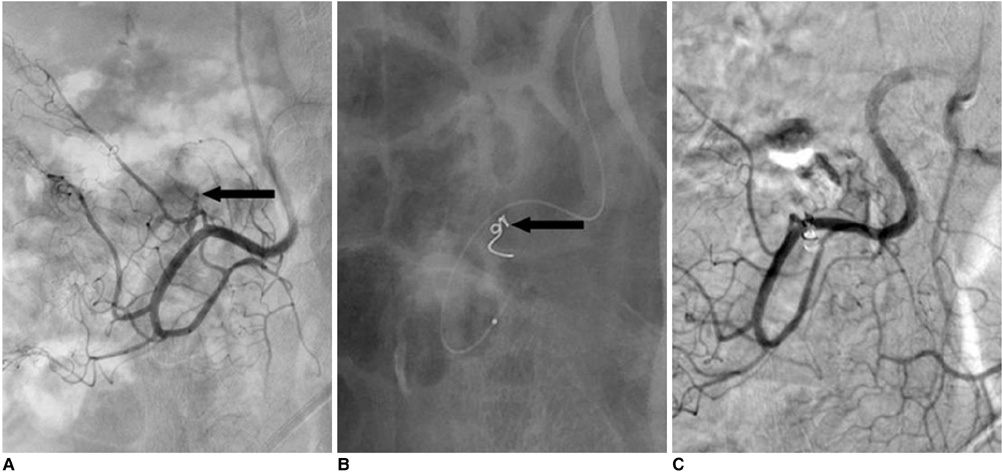
Fig. 2 Results from 81-year-old woman with acute lower gastrointestinal bleeding. A. Selective arteriogram, obtained after coaxial advancement of catheter into right ileocolic artery, shows active hemorrhaging (arrow). B. Branch of right ileocolic artery has been embolized with single 3-2 mm microcoil (arrow). C. Postembolization arteriogram after superselective embolization shows total occlusion of feeding vessel and cessation of hemorrhaging.
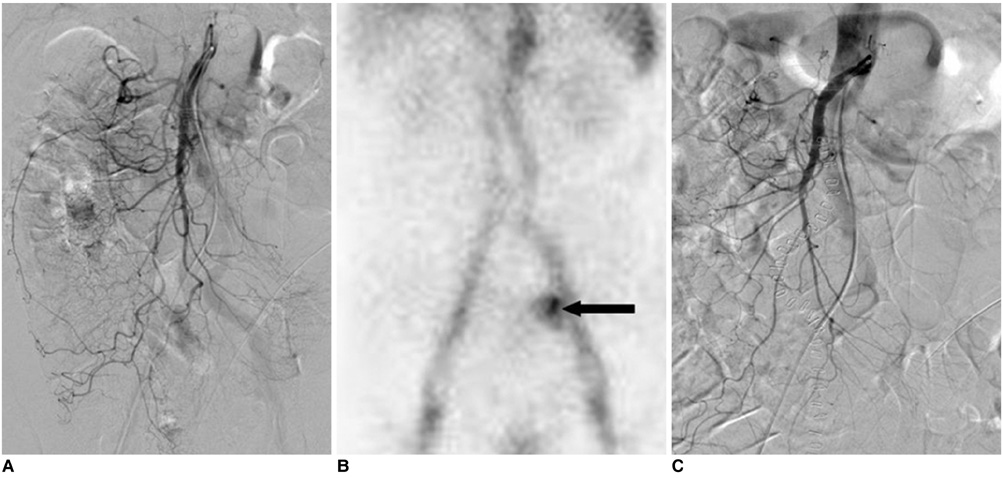
Fig. 3 Results from 69-year-old male patient with acute lower gastrointestinal bleeding following surgical treatment of gastric cancer. A. Superior and inferior mesenteric arteriogram reveals no abnormal extravasation of contrast medium. B. Radionuclide scan with technetium 99m-labeled red blood cells, performed immediately due to continued bleeding, displays bleeding focus (arrow) from increased isotope uptake in left lower quadrant. C. Repeated angiogram does not show extravasation of contrast medium. Patient underwent conservative management and did not show any further bleeding one week later.
Cited by 1 articles
-
Clinical Outcomes of Angiography and Transcatheter Arterial Embolization for Acute Gastrointestinal Bleeding: Analyses according to Bleeding Sites and Embolization Types
Soo Min Noh, Ji Hoon Shin, Ha Il Kim, Sun-Ho Lee, Kiju Chang, Eun Mi Song, Sung Wook Hwang, Dong-Hoon Yang, Byong Duk Ye, Seung-Jae Myung, Suk-Kyun Yang, Jeong-Sik Byeon
Korean J Gastroenterol. 2018;71(4):219-228. doi: 10.4166/kjg.2018.71.4.219.
Reference
-
1. Longstreth GF. Epidemiology and outcome of patients hospitalized with acute lower gastrointestinal hemorrhage: a population-based study. Am J Gastroenterol. 1997. 92:419–424.2. Billingham RP. The conundrum of lower gastrointestinal bleeding. Surg Clin North Am. 1997. 77:241–252.3. Darcy M. Treatment of lower gastrointestinal bleeding: vasopressin infusion versus embolization. J Vasc Interv Radiol. 2003. 14:535–543.4. Zuckerman GR, Prakash C. Acute lower intestinal bleeding: part I. Clinical presentation and diagnosis. Gastrointest Endosc. 1998. 48:606–617.5. Zuckerman GR, Prakash C. Acute lower intestinal bleeding: part II. Etiology, therapy, and outcomes. Gastrointest Endosc. 1999. 49:228–238.6. Gordon RL, Ahl KL, Kerlan RK, Wilson MW, LaBerge JM, Sandhu JS, et al. Selective arterial embolization for the control of lower gastrointestinal bleeding. Am J Surg. 1997. 174:24–28.7. Peck DJ, McLoughlin RF, Hughson MN, Rankin RN. Percutaneous embolotherapy of lower gastrointestinal hemorrhage. J Vasc Interv Radiol. 1998. 9:747–751.8. Defreyne L, Vanlangenhove P, De Vos M, Pattyn P, Van Maele G, Decruyenaere J, et al. Embolization as a first approach with endoscopically unmanageable acute nonvariceal gastrointestinal hemorrhage. Radiology. 2001. 218:739–748.9. Bandi R, Shetty PC, Sharma RP, Burke TH, Burke MW, Kastan D. Superselective arterial embolization for the treatment of lower gastrointestinal hemorrhage. J Vasc Interv Radiol. 2001. 12:1399–1405.10. Waugh J, Madan A, Sacharias N, Thomson K. Embolization for major lower gastrointestinal haemorrhage: five-year experience. Australas Radiol. 2004. 48:311–317.11. d'Othee BJ, Surapaneni P, Rabkin D, Nasser I, Clouse M. Microcoil embolization for acute lower gastrointestinal bleeding. Cardiovasc Intervent Radiol. 2006. 29:49–58.12. Charbonnet P, Toman J, Buhler L, Vermeulen B, Morel P, Becker CD, et al. Treatment of gastrointestinal hemorrhage. Abdom Imaging. 2005. 30:719–726.13. Luchtefeld MA, Senagore AJ, Szomstein M, Fedeson B, Van Erp J, Rupp S. Evaluation of transarterial embolization for lower gastrointestinal bleeding. Dis Colon Rectum. 2000. 43:532–534.14. Burgess AN, Evans PM. Lower gastrointestinal haemorrhage and superselective angiographic embolization. ANZ J Surg. 2004. 74:635–638.15. Drooz AT, Lewis CA, Allen TE, Citron SJ, Cole PE, Freeman NJ, et al. Society of Cardiovascular and Interventional Radiology. Quality improvement guidelines for percutaneous transcatheter embolization: SCVIR Standards of Practice Committee. J Vasc Interv Radiol. 1997. 8:889–895.16. Rockall TA, Logan RF, Devlin HB, Northfield TC. Incidence of and mortality from acute upper gastrointestinal haemorrhage in the United Kingdom. Steering Committee and members of the National Audit of Acute Upper Gastrointestinal Haemorrhage. BMJ. 1995. 311:222–226.17. Kuhle WG, Sheiman RG. Detection of active colonic hemorrhage with use of helical CT: findings in a swine model. Radiology. 2003. 228:743–752.18. Yoon W, Jeong YY, Shin SS, Lim HS, Song SG, Jang NG, et al. Acute massive gastrointestinal bleeding: detection and localization with arterial phase multi-detector row helical CT. Radiology. 2006. 239:160–167.19. Gupta S, Luna E, Kingsley S, Prince M, Herrera N. Detection of gastrointestinal bleeding by radionuclide scintigraphy. Am J Gastroenterol. 1984. 79:26–31.20. Diehl SJ, Ko HS, Dominguez E, Kaare Tesdal I, Kähler G, Böhm C, et al. Negative endoscopy and MSCT findings in patients with acute lower gastrointestinal hemorrhage. Value of (99m) Tc erythrocyte scintigraphy. Radiologe. 2007. 47:64–70.21. Angtuaco TL, Reddy SK, Drapkin S, Harrell LE, Howden CW. The utility of urgent colonoscopy in the evaluation of acute lower gastrointestinal tract bleeding: a 2-year experience from a single center. Am J Gastroenterol. 2001. 96:1782–1785.22. Kusano S, Murata K, Ohuchi H, Motohashi O, Atari H. Low-dose particulate polyvinyl alcohol embolization in massive small artery intestinal hemorrhage. Experimental and clinical results. Invest Radiol. 1987. 22:388–392.23. Han YM, Lee JM, Jin KY, Lee SY, Kim CS. Embolization of superior mesenteric artery branches in dogs. Ischemic bowel changes depend on location of vessel occlusion and embolic materials. Invest Radiol. 1999. 34:629–635.24. Jae HJ, Chung JW, Jung AY, Lee W, Park JH. Transcatheter arterial embolization of nonvariceal upper gastrointestinal bleeding with N-butyl cyanoacrylate. Korean J Radiol. 2007. 8:48–56.25. Setya V, Singer JA, Minken SL. Subtotal colectomy as a last resort for unrelenting unlocalized, lower gastrointestinal hemorrhage: experience with 12 cases. Am Surg. 1992. 58:295–299.26. Ryan JM, Key SM, Dumbleton SA, Smith TP. Nonlocalized lower gastrointestinal bleeding: provocative bleeding studies with intraarterial tPA, heparin, tolazoline. J Vasc Interv Radiol. 2001. 12:1273–1277.27. Johnston C, Tuite D, Pritchard R, Reynolds J, McEniff N, Ryan JM. Use of provocative angiography to localize site in recurrent gastrointestinal bleeding. Cardiovasc Intervent Radiol. 2007. 30:1042–1046.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Outcomes and complications of embolization for gastrointestinal bleeding
- A Case of Massive Bleeding in Jejunal Tuberculosis Treated by Transcatheter Embolization
- The Efficacy and Long-Term Outcome of Microcoil Embolotherapy for Acute Lower Gastrointestinal Bleeding
- Small Bowel Variceal Bleeding in Patients with Liver Cirrhosis Treated with Transarterial Embolization: Case Series
- Is glue embolization safe and effective for gastrointestinal bleeding?
