Diagnostic Value of 3D Fast Low-Angle Shot Dynamic MRI of Breast Papillomas
- Affiliations
-
- 1Department of Radiology, The Research Institute of Radiological Science, Yonsei University College of Medicine, Seoul, Korea. ejsonrd@yuhs.ac
- 2Department of General Surgery, The Research Institute of Radiological Science, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1777100
- DOI: http://doi.org/10.3349/ymj.2009.50.6.838
Abstract
- PURPOSE
To evaluate the value of breast MRI in analysis of papillomas of the breast.
MATERIALS AND METHODS
From 1996 to 2004, 94 patients underwent surgery due to papillomas of the breast. Among them, 21 patients underwent 3D fast low angle shot (FLASH) dynamic breast MRI. Eight masses were palpable and 11 of 21 patients had nipple discharge. Two radiologists indifferently analyzed the location, size of the lesions and shape, margin of the masses, multiplicity and ductal relation. The MRI findings were categorized according to breast imaging reporting and data system (BI-RADS) lexicon. The amount and pattern of enhancement and associated findings were also evaluated according to BI-RADS. We then compared the MRI findings with galactography, mammography and breast ultrasonography (US) and examined histopathologic correlation.
RESULTS
On breast MRI, the lesion size was 0.4-1.59 cm, and 18 patients showed subareolar location. On 4.25 cm (mean 1.54) dynamic enhanced images, imaging findings showed mass (n = 10), intracystic mass (n = 3), focus (n = 5), ductal enhancement (n = 2), and segmental enhancement (n = 1). In cases of the masses, the shapes of the masses were round (n = 4), lobulated (n = 3), and irregular (n = 6), and margins were circumscribed (n = 6), microlobulated (n = 5), and indistinct (n = 2). The enhancement patterns were homogeneous enhancement (n = 7), heterogeneous (n = 3) or rim enhancement (n = 3).
CONCLUSION
The contrast enhanced dynamic breast MRI was highly sensitive for diagnosis of breast papillomas. MRI could play a key role in the pre-operative work-up for multiple papillomas and papillomatosis.
Keyword
MeSH Terms
Figure
-
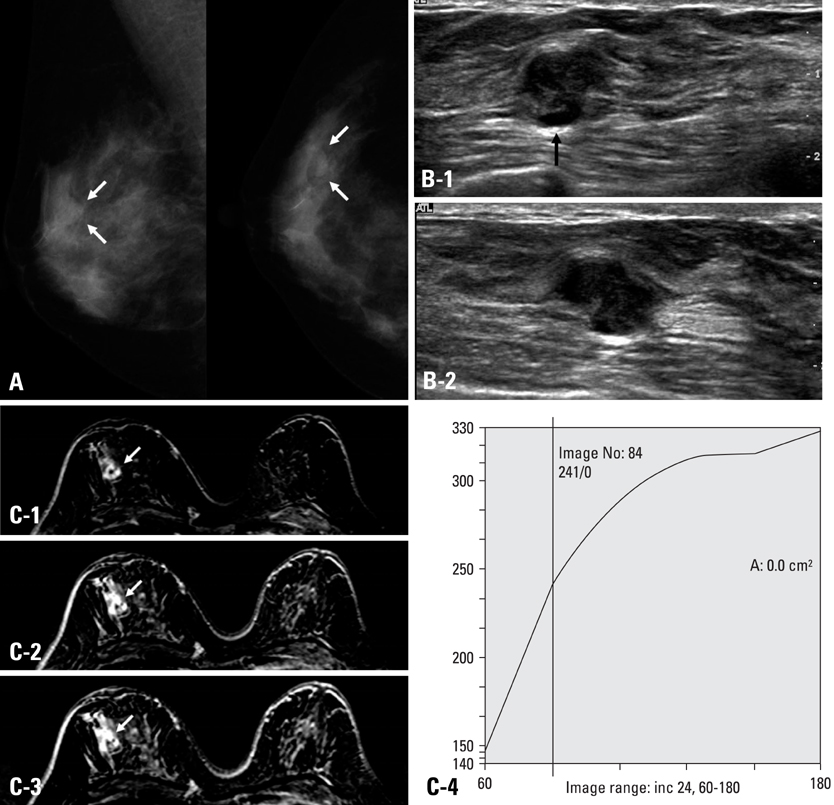
Fig. 1 A 59-year-old woman with palpable mass at 9 : 00 portion of the right breast. She had no symptom of nipple discharge. (A) Right breast mammography showing macolobulated nodule at upper outer area (white arrows). Superficial margin of the mass was obscured. (B) Breast ultrasonography of the mass transverse (1) and longitudinal (2) image revealed isoechoic lobulated mass with some of the margin showing spiculation. Inferior portion of the mass showed dilated duct (arrow in Fig. 1B-1). The sonographic BI-RADS was category 4a, therefore, US-guided core biopsy was recommend. (C) Dynamic contrast breast MRI subtraction 1 minute (1), 3 minutes (2), 5 minutes (3) images. The mass showed lobulated shape, and smooth margin with rim enhancement. Peritumoral delayed enhancement was noted. The kinetics showed persistent enhancement pattern (4). We concluded BI-RADS category 3. The core biopsy and excision were done, and pathologic result was intraductal papilloma.
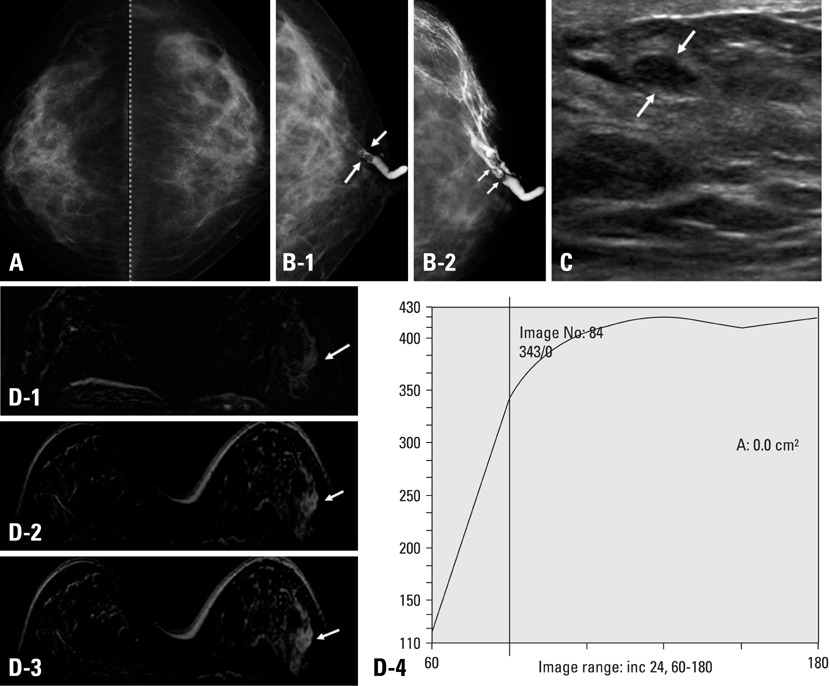
Fig. 2 A 47-year-old woman who had bloody nipple discharge from her left breast for 3 months. (A) Cranial caudal (CC) view of mammography showed heterogeneous dense parenchyma without mass or calcifications. The BI-RADS category was 1, negative finding. (B) Galactography done at left nipple duct revealed intraductal filling defect, and distal portion was not visible (1, white arrows). After injection of more contrast, galactography showed multifocal lobulated filling defects (2, white arrows). (C) Ultrasonography showed focal duct prominency and 0.8 × 0.4 cm sized oval shaped circumscribed nodule with parallel orientation (white arrows), suggesting BI-RADS category 3. (D) Dynamic contrast breast MRI subtraction 1 minute (1), 3 minutes (2), and 5 minutes (3) images demonstrated segmental heterogeneous enhancement. The kinetics showed plateau enhancement pattern (4). We concluded BI-RADS category 4a. Excisional biopsy pathologic result was papillomatosis.

Fig. 3 A 39-year-old woman presented with bloody nipple discharge on her left breast. (A) Left mammography, MLO (1) and CC (2) view showed heterogeneous dense parenchyma pattern and well-circumscribed high density mass lesion at left upper outer portion of breast (white arrow). No evidence of microcalcifications. (B) Breast ultrasonography (a) showed 2.0 × 1.7 cm sized mass lesion at left 2 : 00 portion. The mass was complex cystic mass with internal lobulated hypoechoic solid lesion. Focal ductal extenstion toward the nipple was noted (white arrows). On Doppler image, peripheral increased blood flow was seen. There was no blood flow within the mass (b). (C) On galactography, dilated nipple duct was noted and contrast dye which filled the cystic portion of the mass lesion and solid lesion demonstrated to be lobulated filling defect. (D) Dynamic contrast breast MRI subtraction 1 minute (1), 3 minutes (2), and 5 minutes (3) images. The mass lesion at left 2 : 00 showed peripheral thin rim enhancement. The solid portion of the mass did not reveal enhancement in dynamic images. The enhancement kinetics demonstrated persistent pattern (4), therefore, the BI-RADS category was 3. The pathologic result after excision was intraductal papilloma.
Reference
-
1. Al Sarakbi W, Worku D, Escobar PF, Mokbel K. Breast papillomas: current management with a focus on a new diagnostic and therapeutic modality. Int Semin Surg Oncol. 2006. 3:1.
Article2. Francis A, England D, Rowlands D, Bradley S. Breast papilloma: mammogram, ultrasound and MRI appearances. Breast. 2002. 11:394–397.
Article3. Cardenosa G, Eklund GW. Benign papillary neoplasms of the breast: mammographic findings. Radiology. 1991. 181:751–755.
Article4. Piccoli CW, Feig SA, Vala MA. Breast imaging case of the day. Benign intraductal papilloma with focal atypical papillomatous hyperplasia. Radiographics. 1998. 18:783–786.
Article5. Pisano ED, Braeuning MP, Burke E. Diagnosis please. Case 8: solitary intraductal papilloma. Radiology. 1999. 210:795–798.6. Woods ER, Helvie MA, Ikeda DM, Mandell SH, Chapel KL, Adler DD. Solitary breast papilloma: comparison of mammographic, galactographic, and pathologic findings. AJR Am J Roentgenol. 1992. 159:487–491.
Article7. Krämer SC, Rieber A, Görich J, Aschoff AJ, Tomczak R, Merkle EM, et al. Diagnosis of papillomas of the breast: value of magnetic resonance mammography in comparison with galactography. Eur Radiol. 2000. 10:1733–1736.
Article8. Daniel BL, Gardner RW, Birdwell RL, Nowels KW, Johnson D. Magnetic resonance imaging of intraductal papilloma of the breast. Magn Reson Imaging. 2003. 21:887–892.
Article9. Oyama T, Koerner FC. Noninvasive papillary proliferations. Semin Diagn Pathol. 2004. 21:32–41.10. Dietz JR, Crowe JP, Grundfest S, Arrigain S, Kim JA. Directed duct excision by using mammary ductoscopy in patients with pathologic nipple discharge. Surgery. 2002. 132:582–587.
Article11. Carter D. Intraductal papillary tumours of the breast: a study of 78 cases. Cancer. 1977. 39:1689–1692.
Article12. Haagensen CD, Bodain C, Haagensen DE. Breast carcinoma risk and detection. 1981. Philadelphia: Saunders;146.13. Dupont WD, Page DL. Risk factors for breast cancer in women with proliferative breast disease. N Engl J Med. 1985. 312:46–51.
Article14. Elmore JG, Barton MB, Moceri VM, Polk S, Arena PJ, Fletcher SW. Ten-year risk of false positive screening mammograms and clinical breast examinations. N Engl J Med. 1998. 338:1089–1096.
Article15. Okazaki A, Hirata K, Okazaki M, Svane G, Azavedo E. Nipple discharge disorders: current diagnostic management and the role of fiber-ductoscopy. Eur Radiol. 1999. 9:583–590.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Diagnostic Value of 3D-Gradient Echo Dynamic Contrast Enhanced MRI in Breast Cancer
- Estimation of Pulmonary Motion in Healthy Subjects and Patients with Intrathoracic Tumors Using 3D-Dynamic MRI: Initial Results
- Diagnostic Value of MRI in the T Staging of Colorectal Carcinoma
- MR Imaging of Portal System: Comparison between True-Fast Imaging with Steady State Precession(FISP) and Enhanced Fast Low Angle Shot(FLASH) Imaging
- 3D Whole-Heart Coronary MR Angiography at 1.5T in Healthy Volunteers: Comparison between Unenhanced SSFP and Gd-Enhanced FLASH Sequences
