Male Pseudohermaphroditism Presented with Sudden Cardiac Arrest
- Affiliations
-
- 1Division of Cardiology, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea. cby6908@yuhs.ac
- KMID: 1777005
- DOI: http://doi.org/10.3349/ymj.2012.53.3.658
Abstract
- Torsades de Pointes is a life-threatening arrhythmia associated with a number of causes, but is very rare among endocrinologic disorders. We report a case of male pseudohermaphroditism with hyperaldosteronism due to a 17alpha-hydroxylase deficiency presented with sudden cardiac arrest.
MeSH Terms
Figure
-
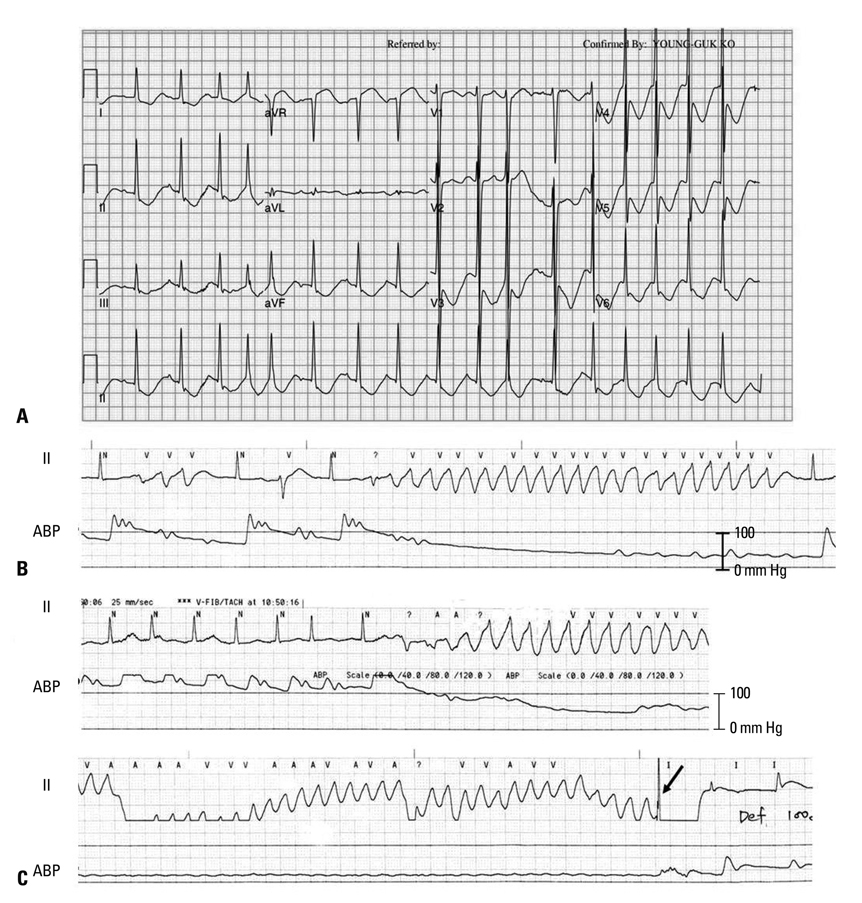
Fig. 1 ECG and arterial blood pressure recording. (A) The 12-lead ECG at the emergency room shows a markedly prolonged QT interval (QTc=635 ms). (B) Spontaneous termination of Torsades de Pointes. Note the short-long-short initiation of polymorphic ventricular tachycardia. (C) Torsades de Pointes with hemodynamic compromise, which was terminated by biphasic shock of 100 J. The ABP waveform became flat after the occurrence of Torsades de Pointes. ABP, arterial blood pressure; ECG, electrocardiogram.

Fig. 2 Abdominal computed tomography showed bilateral hyperplasia of adrenal glands (arrows).
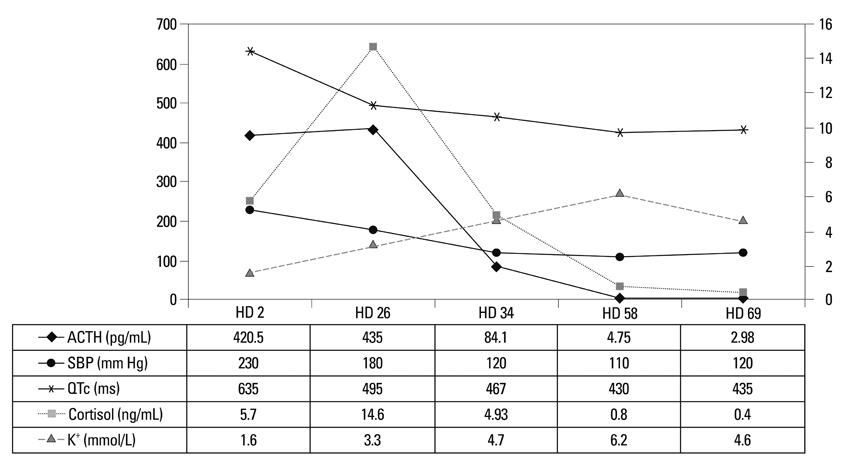
Fig. 3 Clinical course of the patient. Serial variations in plasma ACTH, systolic blood pressure (SBP), corrected QT interval (QTc), serum cortisol, and potassium (K+) are shown. ACTH, adrenocorticotropic hormone; HD, hospital day.
Reference
-
1. Yanase T, Simpson ER, Waterman MR. 17 alpha-hydroxylase/17,20-lyase deficiency: from clinical investigation to molecular definition. Endocr Rev. 1991. 12:91–108.
Article2. Peter M, Sippell WG, Wernze H. Diagnosis and treatment of 17-hydroxylase deficiency. J Steroid Biochem Mol Biol. 1993. 45:107–116.
Article3. Matsumura K, Fujii K, Kansui Y, Arima H, Iida M. Prolongation of the QT interval in primary aldosteronism. Clin Exp Pharmacol Physiol. 2005. 32:66–69.
Article4. Maule S, Mulatero P, Milan A, Leotta G, Caserta M, Bertello C, et al. QT interval in patients with primary aldosteronism and low-renin essential hypertension. J Hypertens. 2006. 24:2459–2464.
Article5. McGowan GK, Walters G. Ventricular arrhythmias and hypokalemia. Lancet. 1976. 2:964.6. Kozhevnikov DO, Yamamoto K, Robotis D, Restivo M, El-Sherif N. Electrophysiological mechanism of enhanced susceptibility of hypertrophied heart to acquired torsade de pointes arrhythmias: tridimensional mapping of activation and recovery patterns. Circulation. 2002. 105:1128–1134.
Article7. Letsas KP, Efremidis M, Kounas SP, Pappas LK, Gavrielatos G, Alexanian IP, et al. Clinical characteristics of patients with drug-induced QT interval prolongation and torsade de pointes: identification of risk factors. Clin Res Cardiol. 2009. 98:208–212.
Article8. Lee SY, Kim JB, Im E, Yang WI, Joung B, Lee MH, et al. A case of catecholaminergic polymorphic ventricular tachycardia. Yonsei Med J. 2009. 50:448–451.
Article9. Gotyo N, Kida M, Horiuchi T, Hirata Y. Torsade de pointes associated with recurrent ampulla cardiomyopathy in a patient with idiopathic ACTH deficiency. Endocr J. 2009. 56:807–815.
Article10. Aydin A, Okmen E, Erdinler I, Sanli A, Cam N. Adrenal adenoma presenting with ventricular fibrillation. Tex Heart Inst J. 2005. 32:85–87.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Medullary Infarction Presenting as Sudden Cardiac Arrest: Report of Two Cases and Review of the Literature
- Cardiac Arrest during Tracheostomy Cannula Misplacement - A Case of Diphtheria
- A Sudden Cardiac Arrest during Spinal Anesthesia
- A Sudden Unexpected Death in Epilepsy
- Cardiac Arrest under Anesthesia in a Child with Previously Undiagnosed Long QT Syndrome: A case report
