Thoracic Endovascular Aortic Repair with the Chimney Technique for Blunt Traumatic Pseudoaneurysm of the Aortic Arch in a No-Option Patient
- Affiliations
-
- 1Division of Cardiology, Eulji University Hospital, Eulji University School of Medicine, Daejeon, Korea. sahnglee@eulji.ac.kr
- 2Division of Chest Surgery, Eulji University Hospital, Eulji University School of Medicine, Daejeon, Korea.
- KMID: 1776948
- DOI: http://doi.org/10.3349/ymj.2013.54.1.258
Abstract
- A 42-year-old man was involved in a motor vehicle collision. Imaging studies revealed the presence of a post-traumatic aortic pseudo-aneurysm (about 34x26 cm) arising from the descending thoracic aorta at the level of the left subclavian artery (LSA), prone to rupture. Thoracic endovascular aneurysm repair (TEVAR) was the only feasible option due to his poor overall medical status. In this case, LSA needed to be covered in order to extend the proximal landing zone. Eventually, modified TEVAR was successfully performed by means of the chimney technique to preserve flow to the LSA and to prevent flow into the pseudoaneurysmal sac.
MeSH Terms
-
Accidents, Traffic
Adult
Aneurysm, False
Aorta, Thoracic/radiography/*surgery
Aortic Aneurysm, Thoracic/radiography/*surgery
Cerebral Hemorrhage/radiography/surgery
Endovascular Procedures/*methods
Humans
Male
Subclavian Artery/radiography/surgery
Tomography, X-Ray Computed
Treatment Outcome
Wounds, Nonpenetrating/radiography/surgery
Figure
-
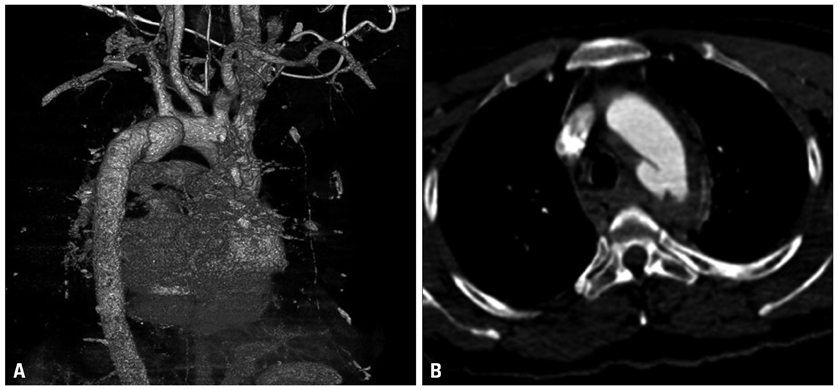
Fig. 1 Pseudoaneurysm and its relationship with surrounding structures. (A) Saccular pseudoaneurysm was noted just distal to the orifice of the LSA on the lesser curvature of the aorta on the three-dimensional reconstruction image of the CT. (B) Axial CT scan showed the presence of a post-traumatic aortic pseudo-aneurysm (about 34×26 cm) arising from the DTA at the level of the LSA. LSA, left subclavian artery; CT, computed tomography; DTA, descending thoracic aorta.

Fig. 2 Endograft deployment resulted in near-total coverage of the LSA (A), followed by retrograde chimney stenting of the LSA origin via the trans-brachial approach (B). The landmark for stent graft placement was the origin of the left CCA. Note that the chimney stent was delivered in advance into the LSA, with protruding into the aortic arch lumen. LSA, left subclavian artery; CCA, common carotid artery.
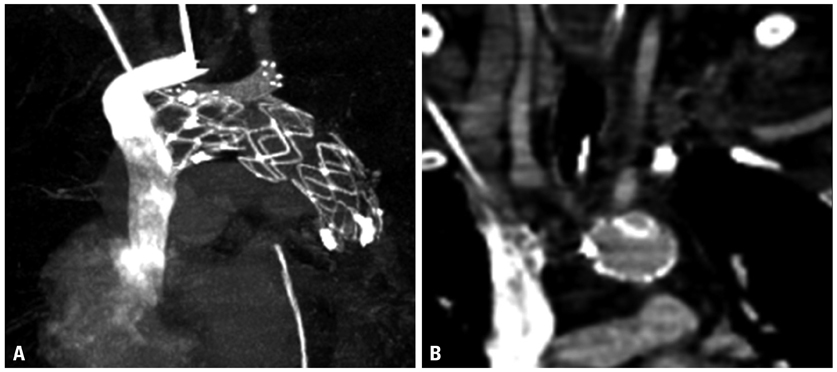
Fig. 3 7 days follow-up CT showing good device morphology and no leakage, patent left CCA, LSA (A), and complete exclusion of the thoracic aortic pseudoaneurysm (B). CT, computed tomography; CCA, common carotid artery; LSA, left subclavian artery.
Reference
-
1. Alla VM, Suryanarayana PG, Thambidorai SK. Thoracic aortic pseudoaneurysm following noncardiovascular surgery: a rare complication that can mimic common chest emergencies. South Med J. 2010. 103:1186–1188.
Article2. Chaikof EL, Mutrie C, Kasirajan K, Milner R, Chen EP, Veeraswamy RK, et al. Endovascular repair for diverse pathologies of the thoracic aorta: an initial decade of experience. J Am Coll Surg. 2009. 208:802–816.
Article3. Kpodonu J, Wheatley GH 3rd, Ramaiah VG, Rodriguez-Lopez JA, Strumpf RK, Diethrich EB. Endovascular repair of an ascending aortic pseudoaneurysm with a septal occluder device: mid-term follow-up. Ann Thorac Surg. 2008. 85:349–351.
Article4. Shim WH. Hybrid approach for complex thoracic aortic pathology. Korean Circ J. 2010. 40:368–369.
Article5. Kang WC, Shin EK, Ahn TH, Lee KH, Moon CI, Han SH, et al. Combined open and endovascular repair for aortic arch pathology. Korean Circ J. 2010. 40:399–404.
Article6. Razzouk A, Gundry S, Wang N, Heyner R, Sciolaro C, Van Arsdell G, et al. Pseudoaneurysms of the aorta after cardiac surgery or chest trauma. Am Surg. 1993. 59:818–823.7. Bizzarri F, Mattia C, Ricci M, Chirichilli I, Santo C, Rose D, et al. Traumatic aortic arch false aneurysm after blunt chest trauma in a motocross rider. J Cardiothorac Surg. 2008. 3:23.
Article8. Woo EY, Carpenter JP, Jackson BM, Pochettino A, Bavaria JE, Szeto WY, et al. Left subclavian artery coverage during thoracic endovascular aortic repair: a single-center experience. J Vasc Surg. 2008. 48:555–560.
Article9. Peterson BG, Eskandari MK, Gleason TG, Morasch MD. Utility of left subclavian artery revascularization in association with endoluminal repair of acute and chronic thoracic aortic pathology. J Vasc Surg. 2006. 43:433–439.
Article10. Reece TB, Gazoni LM, Cherry KJ, Peeler BB, Dake M, Matsumoto AH, et al. Reevaluating the need for left subclavian artery revascularization with thoracic endovascular aortic repair. Ann Thorac Surg. 2007. 84:1201–1205.
Article11. Sugiura K, Sonesson B, Akesson M, Björses K, Holst J, Malina M. The applicability of chimney grafts in the aortic arch. J Cardiovasc Surg (Torino). 2009. 50:475–481.12. Ohrlander T, Sonesson B, Ivancev K, Resch T, Dias N, Malina M. The chimney graft: a technique for preserving or rescuing aortic branch vessels in stent-graft sealing zones. J Endovasc Ther. 2008. 15:427–432.
Article13. Greenberg RK, Clair D, Srivastava S, Bhandari G, Turc A, Hampton J, et al. Should patients with challenging anatomy be offered endovascular aneurysm repair? J Vasc Surg. 2003. 38:990–996.
Article14. Criado FJ. A percutaneous technique for preservation of arch branch patency during thoracic endovascular aortic repair (TEVAR): retrograde catheterization and stenting. J Endovasc Ther. 2007. 14:54–58.
Article15. Hiramoto JS, Schneider DB, Reilly LM, Chuter TA. A double-barrel stent-graft for endovascular repair of the aortic arch. J Endovasc Ther. 2006. 13:72–76.16. Feng R, Zhao Z, Bao J, Wei X, Wang L, Jing Z. Double-chimney technology for treating secondary type I endoleak after endovascular repair for complicated thoracic aortic dissection. J Vasc Surg. 2011. 54:212–215.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Modified Chimney Technique With a Thoracic Aortic Stent Graft to Preserve the Blood Flow of the Left Common Carotid Artery for Treating Descending Thoracic Aortic Aneurysm and Dissection
- Endovascular Repair of a Juxtarenal Abdominal Aortic Aneurysm Using a Chimney Graft
- Off-the-Shelf, Hybrid, Innominate Chimney Thoracic Endovascular Aneurysm Repair for Treatment of Mycotic Thoracic Aortic Aneurysm: A Case Report
- Thoracic Endovascular Repair by Chimney Technique for Aortic Dissection with Malperfusion Syndrome
- Blunt Aortic Injury: Changing the First Treatment Modality
