Recanalization of a Coronary Chronic Total Occlusion by a Retrograde Approach Using Ipsilateral Double Guiding Catheters
- Affiliations
-
- 1Division of Cardiology, Department of Medicine, Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicine, Bucheon, Korea. naeheelee@paran.com
- KMID: 1769513
- DOI: http://doi.org/10.4070/kcj.2009.39.1.42
Abstract
- The retrograde approach through a collateral artery is now thought to improve the success rate of percutaneous coronary intervention (PCI) for coronary chronic total occlusion (CTO), and different kinds of strategies for this technique have been developed. However, the basic principles of PCI for CTO, such as firm back-up support with a guiding catheter and fine control of the guide wire, should be adhered to more strictly to succeed with this complex procedure. We present a case in which a CTO of the proximal left anterior descending artery was successfully opened by the retrograde approach through a collateral from the left circumflex artery, during which two guiding catheters were simultaneously used in the same coronary artery for the purpose of strong back up support for the retrograde device and fine control for the antegrade device.
MeSH Terms
Figure
-

Fig. 1 Baseline coronary angiography. A and B: left coronary angiography showed chronic total occlusion at the trifurcation site of the proximal left anterior descending artery. An epicardial collateral connection between the distal left circumflex coronary artery and distal left anterior descending artery was observed (arrow). C: the right coronary artery was diminutive and provided the collateral flow to the left anterior descending artery through the cornus branch.
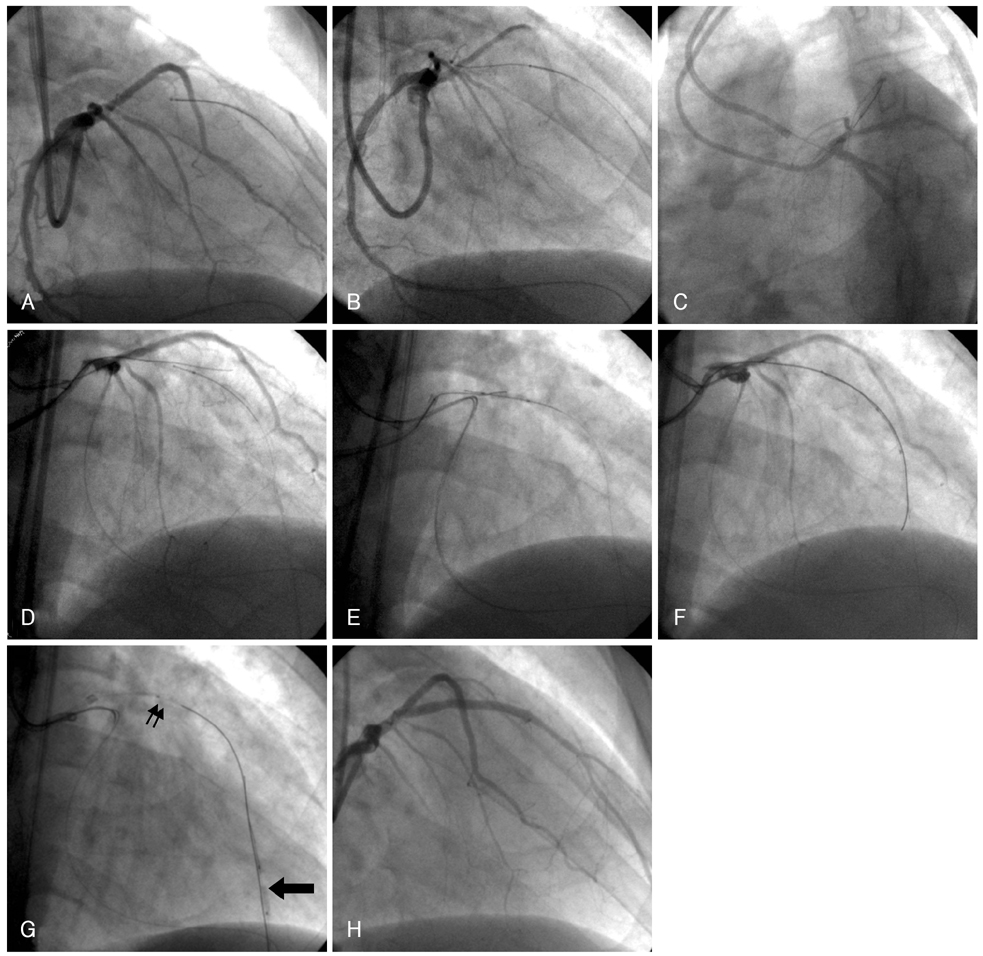
Fig. 2 Retrograde approach for chronic total occlusion. A: a Fielder FC wire supported by a 150 cm Progreat microcatheter was successfully introduced distal to the chronic total occlusion. B: the retrograde wires could not puncture the proximal cap correctly and these wires repeatedly entered the subintimal space proximal to the chronic total occlusion (failed retrograde wire crossing technique). C: another guiding catheter (6 Fr JL-4 SH) was engaged into the left coronary artery for better manipulability of the antegrade wire, while keeping the previous Amplatz guiding catheter located near the left coronary artery ostium. D: the Kissing wire technique was unsuccessful. E, F: controlled antegrade and retrograde subintimal tracking (CART) technique was applied; after retrograde ballooning (2.0×20 mm) was performed at the chronic total occlusion site, including the site distal to the chronic total occlusion, the Miracle 12 g wire could be passed into the distal true lumen. G: the passed antegrade Miracle 12 g wire was anchored by the retrograde ballooning (arrow) in order to facilitate the antegrade balloon (double arrows) passage (distal anchoring balloon technique). H: final angiography after placement of two Taxus stents.
Reference
-
1. Hoye A, van Domgurg RT, Sonnenschien K, Serruys PW. Percutaneous coronary intervention for chronic total occlusions: the thoraxcenter experience 1992-2002. Eur Heart J. 2005. 26:2630–2636.2. Choi RK, Won KW, Moon KS, et al. Result of percutaneous transluminal coronary angioplasty of chronic total occlusion. Korean Circ J. 2000. 30:416–423.3. Saito S, Tanaka S, Hiroe Y, et al. Angioplasty for chronic total occlusion by using tapered-tip guidewires. Catheter Cardiovasc Interv. 2003. 59:305–311.4. Lee NH, Cho YH, Seo HS. Successful recanalization of in-stent coronary chronic total occlusion by subintimal tracking. J Invasive Cardiol. 2008. 20:E129–E132.5. Hirokami M, Saito S, Muto H. Anchoring technique to improve guiding catheter support in coronary angioplasty of chronic total occlusion. Catheter Cardiovasc Interv. 2006. 67:366–371.6. Surmely JF, Tsuchikane E, Katoh O, et al. New concept for CTO recanalization using controlled antegrade and retrograde subintimal tracking. J Invasive Cardiol. 2006. 18:334–338.7. Saito S. Different strategies of retrograde approach in coronary angioplasty for chronic total occlusion. Catheter Cardiovasc Interv. 2008. 71:8–19.8. Kukreja N, Serruys PW, Sianos G. Retrograde recanalization of chronically occluded coronary arteries: illustration and description of the technique. Catheter Cardiovasc Interv. 2007. 69:833–841.9. Ozawa N. A new understanding of chronic total occlusion from a novel PCI technique that involves a retrograde approach to the right coronary artery via a septal branch and passing of the guidewire to a guiding catheter on the other side of lesion. Catheter Cardiovasc Interv. 2006. 68:907–913.10. Kahn JK, Hartzler GO. Retrograde coronary angioplasty of isolated arterial segments through saphenous vein bypass grafts. Cathet Cardiovasc Diagn. 1990. 20:88–93.11. Stone GW, Colombo A, Teirstein PS, et al. Percutaneous recanalization of chronically occluded coronary arteries: procedural techniques, devices, and results. Catheter Cardiovasc Interv. 2005. 66:217–236.12. Kim JY, Yoon JH, Jung HS, et al. The experience of transradial coronary intervention for chronic total occlusion. Korean Circ J. 2003. 33:805–812.13. Noguchi T, Miyazaki S, Morii I, Daikoku S, Goto Y, Nonogi H. Percutaneous transluminal coronary angioplasty of chronic total occlusions: determinants of primary success and long-term clinical outcome. Catheter Cardiovasc Interv. 2000. 49:258–264.14. Surmely JF, Katoh O, Tsuchikane E, Nasu K, Suzuki T. Coronary septal collaterals as an access for the retrograde approach in the percutaneous treatment of coronary chronic total occlusions. Catheter Cardiovasc Interv. 2007. 69:826–832.15. Matsumi J, Saito S. Progress in the retrograde approach for chronic total coronary artery occlusion: a case with successful angioplasty using CART and reverse-anchoring techniques 3 years after failed PCI via a retrograde approach. Catheter Cardiovasc Interv. 2008. 71:810–814.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Iteration of Reverse Controlled Antegrade and Retrograde Tracking for Coronary Chronic Total Occlusion Intervention: a Current Appraisal
- Strategies for Successful Percutaneous Revascularization of Chronic Total Occlusion of the Femoropopliteal Arteries When the Antegrade Passage of a Guide Wire Fails
- Changes in Coronary Perfusion after Occlusion of Coronary Arteries in Kawasaki Disease
- The Experience of Transradial Coronary Intervention for Chronic Total Occlusion
- The Feasibility of Percutaneous Transradial Coronary Intervention for Chronic Total Occlusion
