Current Mechanical Circulatory Support Devices for End Stage Heart Failure
- Affiliations
-
- 1Department of Cardiovascular Surgery, Yonsei Cardiovascular Hospital, Yonsei University Health System, Seoul, Korea. yhpark@yuhs.ac
- KMID: 1769506
- DOI: http://doi.org/10.4070/kcj.2009.39.1.1
Abstract
- Mechanical circulatory support is necessary when heart failure becomes refractory to medical support. It is typically instituted when organ dysfunction occurs as a result of hypoperfusion. Enthusiasm has recently developed for the role of mechanical circulatory support in the ever-growing population of heart failure patients. Indeed, efforts in developing this technology have allowed for the relatively recent development of a variety of complete circulatory support devices. The use of left ventricular assist devices (LVADs) in patients with advanced heart failure results in a clinically meaningful survival benefit and an improved quality of life, and LVADs could be an acceptable alternative therapy for selected patients who are not candidates for cardiac transplantation.
MeSH Terms
Figure
-

Fig. 1 Device selection. RHF: right heart failure, TAH: total artificial heart, CHF: congestive heart failure, LV: left ventricle.7)
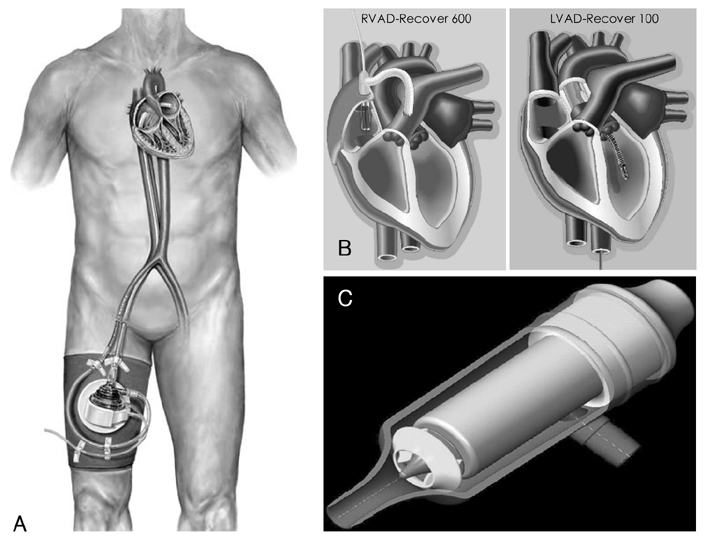
Fig. 2 The TandemHeart System is a cardiac support system that is deployed percutaneously. For left heart support, the left atrium is accessed via the femoral vein using a transseptal puncture. Device outflow is directed into the femoral artery. The system can be used either in the cardiac catheterization laboratory or in the operating room (A). The Impella Recover Device is inserted percutaneously and positioned within the left ventricle (LVAD-Recover 100), and the RVAD-Recover 600 is positioned between the right atrium and pulmonary artery for inflow and outflow (B). MEDOS DeltaStream DP1 features a diagonal-flow impeller and can be used for both continuous and pulsatile output (C). LVAD: left ventricular assist device, RVAD: right ventricular assist device.
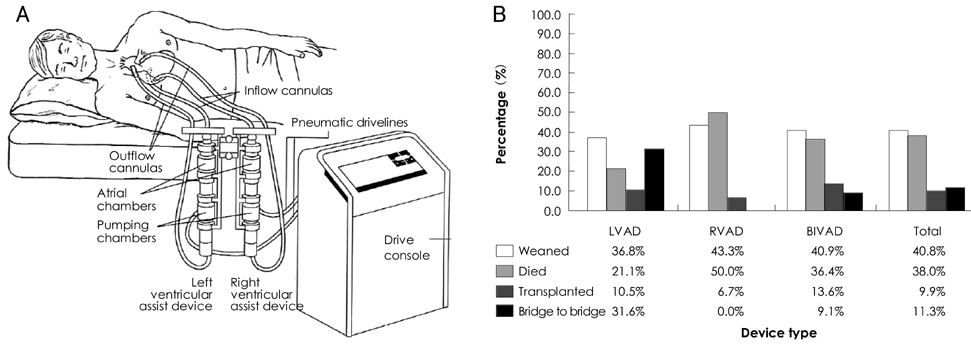
Fig. 3 The Abiomed BVS 5000 is a dual chamber, pulsatile ventricular assist device and used for isolated univentricular or biventricular support. A: the AbioMed BVS 5000. Both the pumps and drive consoles are external. B: outcomes after Abiomed BVS 5000 implantation. LVAD: left ventricular assist device, RVAD: right ventricular assist device, BIVAD: biventricular assist device.
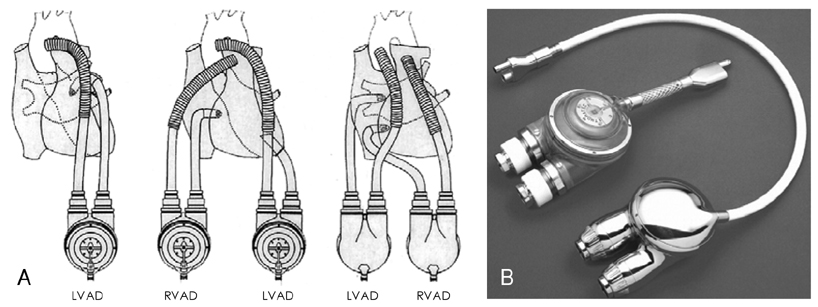
Fig. 4 Thoratec VAD is a pneumatically driven device and modified for implantation. A: variable options and configurations for implantation of the Thoratec VAD. B: the right photo shows the device was modified as a Thoratec IVAD for implantation. LVAD: left ventricular assist device, RVAD: right ventricular assist device.

Fig. 5 A: Berlin Heart Excor pumps with 10 mL and 80 mL stroke volumes. B: Cross-section of the Berlin Heart Pump. Various sizes of MEDOS MCSDs (right). MCSDs: mechanical circulatory support devices.
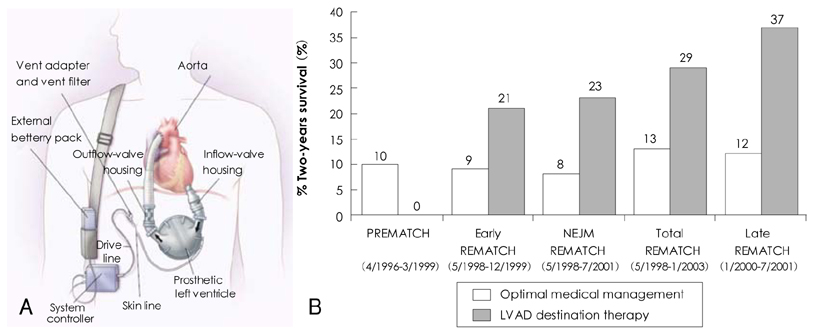
Fig. 6 HeartMate XVE implantable device (A) and improved two-year survival rates (B). The figure shows improved two-year survival rates in the "LVAD as Destination Therapy" patients enrolled during the second half of the REMATCH trial, compared with the unchanged outcomes in medical therapy patients during the trial.15) LVAD: left ventricular assist device, REMATCH: Randomized Evaluation of Mechanical Assistance for the Treatment of Congestive Heart Failure.
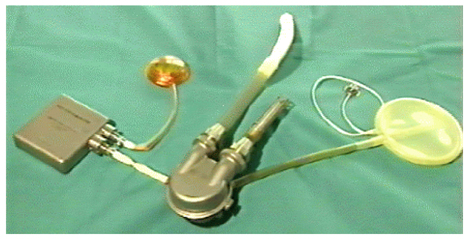
Fig. 7 The Arrow LionHeart is the first fully implantable pulsatile LVAD. It removes the need for a percutaneous driveline, greatly reducing the infection risk and allowing the recipient the flexibility of being completely untethered for periods of up to 40 minutes. LVAD: left ventricular assist device.
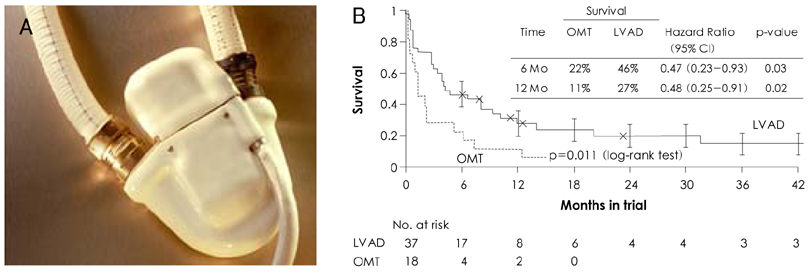
Fig. 8 The NovaCor electrical implanted LVAD was designed, from the outset, as a permanent solution to end-stage heart disease. The pump is implanted below the diaphragm and drains the left ventricle by way of a valved apical conduit. Blood is returned to the ascending aorta. Power and control lines are connected via a vented percutaneous driveline. The patient wears an electronic controller and two power packs, which allow up to seven hours of tether-free operation (A). Survival at 6 months and 12 months demonstrates an approximate 50% reduction in the risk of death at these time points. Kaplan-Meier survival curves are also shown. The x represents censoring at the time of transplantation (B).17) LVAD: left ventricular assist device, INTrEPID: investigation of non-transplant eligible patients who are inotrope-dependent, OMT: optimal medical therapy.
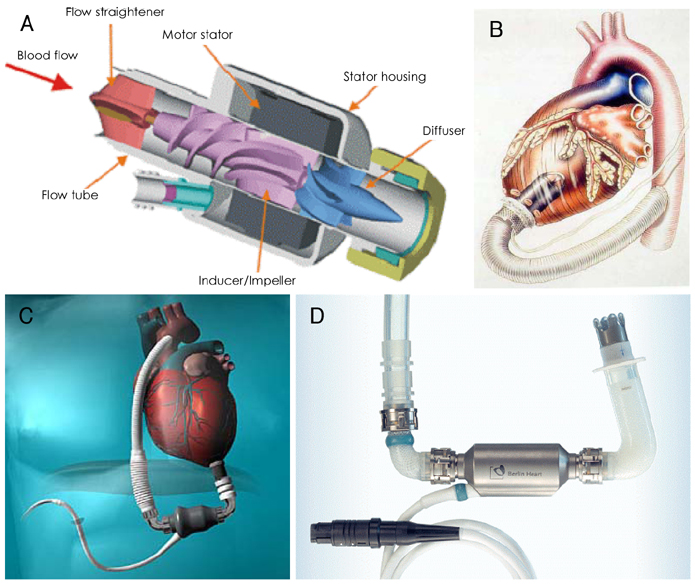
Fig. 9 Axial Flow Pumps. A: MicroMed DeBakey VAD. B: the Jarvik 2000 FlowMaker is an axial-flow device that is positioned within the left ventricle. The device can be configured for either a percutaneous or postauricular power delivery system. C: the HeartMate II LVAS is an axial flow pump that withdraws blood from the left ventricular apex and returns it to the ascending aorta. The system is implanted in a manner quite similar to that employed with the pulsatile HeartMate I LVAS. The blood pump is powered by two external battery packs and a system controller. D: the Berlin Heart InCor is a second generation axial pump that employs a magnetically suspended impeller, making for enhanced potential durability. VAD: ventricular assist device, LVAS: left ventricular assist system.

Fig. 10 Various third generation centrifugal pump models. A: EvaHeart. B: DuraHeart. C: HeartMate III. D: the CorAide LVAS is a third-generation centrifugal pump. The blood-lubricated fluid film bearing washes the space between the suspended rotating and stationary stator assemblies. The implanted blood pump is powered by an external electric subsystem consisting of a rechargeable battery and a portable electronic module (PEM). E: the rotor in the VentrAssist LVAS blood pump is fully washed and hydrodynamically suspended. The blood-contacting surfaces are covered with a diamond-like carbon coating to reduce platelet adhesion. Patients are required to take both aspirin and warfarin. F: HeartWare. LVAS: left venticular assist system.
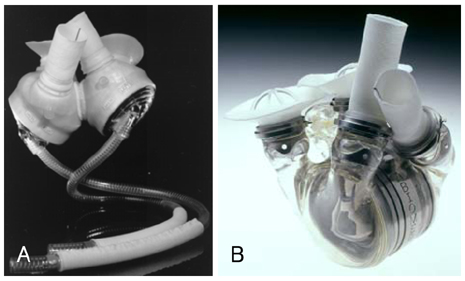
Fig. 11 The CardioWest Total Artificial Heart (Syncardia Systems, Inc) (A) and the AbioCor Total Artificial Heart (Abiomed, Inc) were the first fully implantable BIVADs. The heart is placed orthotopically, and the TETS, controller, and rechargeable battery pack are implanted within the abdominal space. TETS: transcutaneous energy transfer system (B). BIVAD: biventricular assist device.
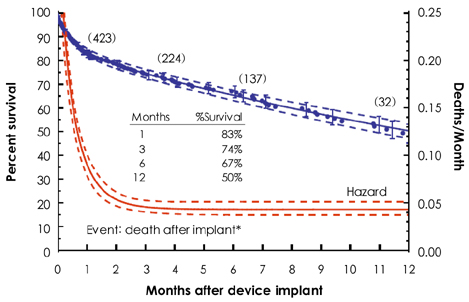
Fig. 12 Survival curve and accompanying hazard function for ISHLT/MCSD analysis, January 2002 to December 2004 (n=655; 178 total deaths). MCSD: mechanical circulatory support device, ISHLT: International Society of Heart and Lung Transplantion.
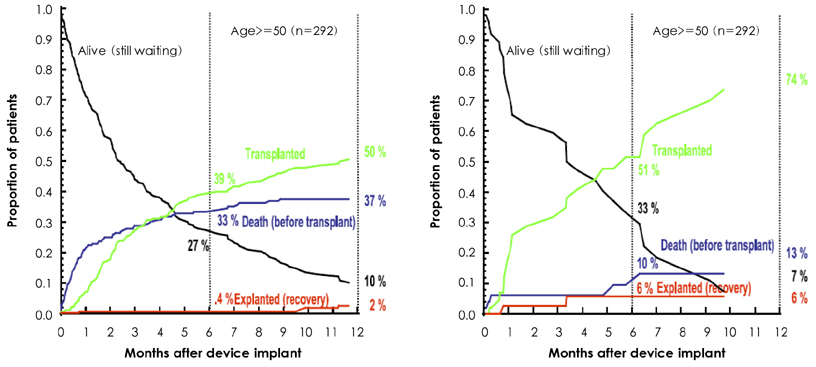
Fig. 13 Outcomes of mutually exclusive events after device implantation among patients receiving mechanical circulatory support device therapy as a bridge to transplantation. The depictions are stratified according to age at implantation. At any point in time, the sum of the probabilities of each event equals 100%. The depiction on the left is for patients ≧50 years of age. For patients <30 years of age (shown on the right), the data suggest that bridging was extremely successful. ISHLT/MCSD analysis, January 2002 to December 2004. ISHLT: International Society of Heart and Lung Transplantion, MCSD: mechanical circulatory support devices.
Cited by 1 articles
-
Pediatric Ventricular Assist Device
Yu Rim Shin, Young-Hwan Park, Han Ki Park
Korean Circ J. 2019;49(8):678-690. doi: 10.4070/kcj.2019.0163.
Reference
-
1. DeBakey ME. Development of mechanical heart devices. Ann Thorac Surg. 2005. 79:S2228–S2231.2. DeBakey ME. Left ventricular bypass pump for cardiac assistance: clinical experience. Am J Cardiol. 1971. 27:3–11.3. Cooley DA, Liotta D, Hallman GL, Bloodwell RD, Leachman RD, Milam JD. Orthotopic cardiac prosthesis for two staged cardiac replacement. Am J Cardiol. 1969. 24:723–730.4. Heart Disease and Stroke Statistics: 2004 update. 2004. Dallas: American Heart Association;24–25.5. Hochman JS, Buller CE, Sleeper LA, et al. Cardiogenic shock complicating acute myocardial infarction: etiologies, management and outcome. J Am Coll Cardiol. 2000. 36:3 Suppl A. 1063–1070.6. Wheeldon DR. Mechanical circulatory support: state of the art and future perspectives. Perfusion. 2003. 18:233–243.7. DiGiorgi P, Rao V, Naka Y, Oz M. Which patient, which pump? J Heart Lung Transplant. 2003. 22:221–235.8. Deng MC, Naka Y. Mechanical Circulatory Support Therapy in Advanced Heart Failure. 2007. London: Imperial College Press;40–69.9. Chandra D, Kar B, Idelchik G, et al. Usefulness of percutaneuous left ventricular assist device as a bridge to recovery from myocarditis. Am J Cardiol. 2007. 99:1755–1756.10. Siegenthaler MP, Brehm K, Strecker T, et al. The Impella Recover microaxial left ventricular assist device reduces mortality for postcardiotomy failure: a three-center experience. J Thorac Cardiovasc Surg. 2004. 127:812–822.11. Agati S, Ciccarello G, Ocello S, et al. Pulsatile ECMO and VAD: a dual use of a new device in pediatric cardiac patients. ASAIO J. 2006. 52:501–504.12. Morgan JA, Stewart AS, Lee BJ, Oz MC, Naka Y. Role of the Abiomed BVS 5000 device for short-term support and bridge to transplantation. ASAIO J. 2004. 50:360–363.13. Magliato K, Kleisli T, Soukiasian H, et al. Biventricular support in patients with profound cardiogenic shock: single center experience. ASAIO J. 2003. 49:475–479.14. Rose EA, Gelijns AC, Moskowitz AJ, et al. Long-term mechanical left ventricular assistance for end-stage heart failure. N Engl J Med. 2001. 345:1435–1443.15. Leitz K, Miller LW. Will left-ventricular assist device therapy replace heart transplantation in the foreseeable future? Curr Opin Cardiol. 2005. 20:132–137.16. Pae WE, Connell JM, Adelowo A, et al. Does total implantability reduce infection with the use of a left ventricular assist device? J Heart Lung Transplant. 2007. 26:219–229.17. Rogers JG, Butler J, Lansman SL, et al. Chronic mechanical circulatory support for inotrope-depedent heart failure patients who are not transplant candidates. J Am Coll Cardiol. 2007. 50:741–747.18. Deng MC, Edwards LB, Hertz MI, et al. Mechanical circulatory support device database of the International Society for Heart and Lung Transplantation: third annual report-2005. J Heart Lung Transplant. 2005. 24:1182–1187.19. McMurray JJ, Stewart S. Epidemiology, aetiology and prognosis of heart failure. Heart. 2000. 83:596–602.20. Hosenpud JD, Bennett LE, Keck BM, Boucek MM, Novick RJ. The Registry of the International Society for Heart and Lung Transplantation: eighteenth official report-2001. J Heart Lung Transplant. 2001. 20:805–815.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of Advanced Heart Failure: Beyond Medical Treatment
- Pediatric Mechanical Circulatory Support
- Mechanical Circulatory Support for Advanced Heart Failure
- Treatment of Medically Intractable End-Stage Heart Failure
- Short-term Mechanical Circulatory Support with Centrifugal Pump in Cardiac Arrest or Cardiogenic Shock: Report of 5 cases
