J Korean Soc Menopause.
2013 Apr;19(1):18-25. 10.6118/jksm.2013.19.1.18.
Discrimination between Benign and Malignant Pelvic Masses Using the Risk of Malignancy Index 1
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Inha University College of Medicine, Incheon, Korea. songsong2000@gmail.com
- KMID: 1768793
- DOI: http://doi.org/10.6118/jksm.2013.19.1.18
Abstract
OBJECTIVES
To assess the ability of risk of malignancy index (RMI) 1 to discriminate between benign and malignant pelvic masses.
METHODS
Between January 2007 and December 2010, 547 women with pelvic masses were evaluated. Their medical records are reviewed here retrospectively. The sensitivity, specificity and positive and negative predictive values of the cancer antigen (CA) 125 level, ultrasound findings and menopausal status in the prediction of malignant pelvic masses were calculated and compared individually or combined using the RMI 1.
RESULTS
The receiver operating characteristic (ROC) curves of CA 125, the ultrasound score and the RMI 1 were all found to be relevant predictors of malignancy. ROC analysis of the RMI 1, CA 125 serum levels, ultrasound score and menopausal status showed areas under the curves of 0.795, 0.782, 0.784 and 0.594, respectively. The RMI 1 was found to be statistically significantly correlated with menopausal status (P = 0.001), while not statistically significantly correlated with CA 125 (P = 0.628) or the ultrasound score (P = 0.541). The RMI 1 at a cut-off of 150 - with a sensitivity of 77.9%, specificity of 81.1%, positive predictive value of 51.7% and negative predictive value of 93.4% - showed the highest performance in determining the malignant tendency of pelvic masses.
CONCLUSION
Accepting a RMI 1 cut-off value of 150 results in statistically more significant diagnostic criteria than menopausal status for the discrimination of benign and malignant pelvic masses.
Keyword
MeSH Terms
Figure
-
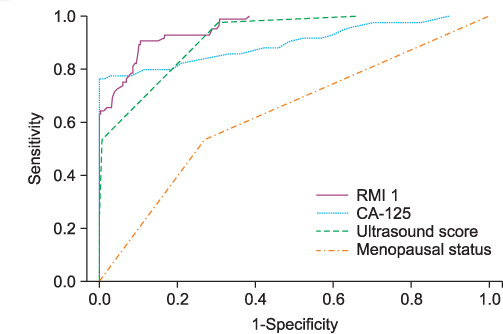
Fig. 1 Receiver operating characteristic (ROC) curves of individual predictors showing the relationship between sensitivity and specificity of menopause score, ultrasound score, serum cancer antigen (CA) 125 level and the risk of malignancy index (RMI) 1 in the discrimination between benign and malignant pelvic masses.
Reference
-
1. Young RC, Decker DG, Wharton JT, Piver MS, Sindelar WF, Edwards BK, et al. Staging laparotomy in early ovarian cancer. JAMA. 1983. 250:3072–3076.2. Gillis CR, Hole DJ, Still RM, Davis J, Kaye SB. Medical audit, cancer registration, and survival in ovarian cancer. Lancet. 1991. 337:611–612.3. Engelen MJ, Kos HE, Willemse PH, Aalders JG, de Vries EG, Schaapveld M, et al. Surgery by consultant gynecologic oncologists improves survival in patients with ovarian carcinoma. Cancer. 2006. 106:589–598.4. Earle CC, Schrag D, Neville BA, Yabroff KR, Topor M, Fahey A, et al. Effect of surgeon specialty on processes of care and outcomes for ovarian cancer patients. J Natl Cancer Inst. 2006. 98:172–180.5. Kumpulainen S, Kuoppala T, Leminen A, Penttinen J, Puistola U, Pukkala E, et al. Surgical treatment of ovarian cancer in different hospital categories--a prospective nation-wide study in Finland. Eur J Cancer. 2006. 42:388–395.6. Goff BA, Matthews BJ, Wynn M, Muntz HG, Lishner DM, Baldwin LM. Ovarian cancer: patterns of surgical care across the United States. Gynecol Oncol. 2006. 103:383–390.7. Jacobs I, Oram D, Fairbanks J, Turner J, Frost C, Grudzinskas JG. A risk of malignancy index incorporating CA 125, ultrasound and menopausal status for the accurate preoperative diagnosis of ovarian cancer. Br J Obstet Gynaecol. 1990. 97:922–929.8. Tingulstad S, Hagen B, Skjeldestad FE, Onsrud M, Kiserud T, Halvorsen T, et al. Evaluation of a risk of malignancy index based on serum CA125, ultrasound findings and menopausal status in the pre-operative diagnosis of pelvic masses. Br J Obstet Gynaecol. 1996. 103:826–831.9. Tingulstad S, Hagen B, Skjeldestad FE, Halvorsen T, Nustad K, Onsrud M. The risk-of-malignancy index to evaluate potential ovarian cancers in local hospitals. Obstet Gynecol. 1999. 93:448–452.10. Davies AP, Jacobs I, Woolas R, Fish A, Oram D. The adnexal mass: benign or malignant? Evaluation of a risk of malignancy index. Br J Obstet Gynaecol. 1993. 100:927–931.11. Morgante G, la Marca A, Ditto A, De Leo V. Comparison of two malignancy risk indices based on serum CA125, ultrasound score and menopausal status in the diagnosis of ovarian masses. Br J Obstet Gynaecol. 1999. 106:524–527.12. Aslam N, Tailor A, Lawton F, Carr J, Savvas M, Jurkovic D. Prospective evaluation of three different models for the pre-operative diagnosis of ovarian cancer. BJOG. 2000. 107:1347–1353.13. Manjunath AP, Pratapkumar , Sujatha K, Vani R. Comparison of three risk of malignancy indices in evaluation of pelvic masses. Gynecol Oncol. 2001. 81:225–229.14. Mol BW, Boll D, De Kanter M, Heintz AP, Sijmons EA, Oei SG, et al. Distinguishing the benign and malignant adnexal mass: an external validation of prognostic models. Gynecol Oncol. 2001. 80:162–167.15. Torres JC, Derchain SF, Faundes A, Gontijo RC, Martinez EZ, Andrade LA. Risk-of-malignancy index in preoperative evaluation of clinically restricted ovarian cancer. Sao Paulo Med J. 2002. 120:72–76.16. Andersen ES, Knudsen A, Rix P, Johansen B. Risk of malignancy index in the preoperative evaluation of patients with adnexal masses. Gynecol Oncol. 2003. 90:109–112.17. Obeidat BR, Amarin ZO, Latimer JA, Crawford RA. Risk of malignancy index in the preoperative evaluation of pelvic masses. Int J Gynaecol Obstet. 2004. 85:255–258.18. Bailey J, Tailor A, Naik R, Lopes A, Godfrey K, Hatem HM, et al. Risk of malignancy index for referral of ovarian cancer cases to a tertiary center: does it identify the correct cases? Int J Gynecol Cancer. 2006. 16:Suppl 1. 30–34.19. Ulusoy S, Akbayir O, Numanoglu C, Ulusoy N, Odabas E, Gulkilik A. The risk of malignancy index in discrimination of adnexal masses. Int J Gynaecol Obstet. 2007. 96:186–191.20. Yamamoto Y, Yamada R, Oguri H, Maeda N, Fukaya T. Comparison of four malignancy risk indices in the preoperative evaluation of patients with pelvic masses. Eur J Obstet Gynecol Reprod Biol. 2009. 144:163–167.21. FIGO Cancer Committee. Staging announcement. Gynecol Oncol. 1986. 25:383–385.22. Strigini FA, Gadducci A, Del Bravo B, Ferdeghini M, Genazzani AR. Differential diagnosis of adnexal masses with transvaginal sonography, color flow imaging, and serum CA 125 assay in pre- and postmenopausal women. Gynecol Oncol. 1996. 61:68–72.23. Yazbek J, Aslam N, Tailor A, Hillaby K, Raju KS, Jurkovic D. A comparative study of the risk of malignancy index and the ovarian crescent sign for the diagnosis of invasive ovarian cancer. Ultrasound Obstet Gynecol. 2006. 28:320–324.24. Alanbay I, Akturk E, Coksuer H, Ercan M, Karaşahin E, Dede M, et al. Comparison of risk of malignancy index (RMI), CA125, CA 19-9, ultrasound score, and menopausal status in borderline ovarian tumor. Gynecol Endocrinol. 2012. 28:478–482.25. Cho IS, Nam KH, Lee HH, Kim JS, Kim TH, Cho HJ, et al. A new scoring system for differentiation between benign and malignant ovarian masses. Korean J Obstet Gynecol. 2006. 49:1681–1689.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Four risk of malignancy indices in evaluation of pelvic masses
- The effectiveness and limitations of the Risk of Malignancy Index in evaluation of adnexal masses
- The Usefulness of Scoring System Distinguishing between Benign and Malignant Breast Masses on Ultrasonogram
- Comparison of the Usefulness of four Risk-of-Malignancy Indices using Ultrasonography in Ovarian masses
- Comparison of four malignancy risk indices in the detection of malignant ovarian masses
