Initial Experience with Percutaneous Needle Aspiration of Paraspinal Lesions Using XperGuide Cone-Beam CT
- Affiliations
-
- 1Department of Radiology, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea. parkhiji@gmail.com
- KMID: 1748459
- DOI: http://doi.org/10.3348/jksr.2013.68.3.245
Abstract
- PURPOSE
The aim of this study is to report our initial experience using XperGuide cone-beam computed tomography (CBCT) for percutaneous needle aspiration of the paraspinal lesions.
MATERIALS AND METHODS
Between September 2011 and September 2012, 12 patients who underwent percutaneous needle aspiration of the paraspinal lesions for suspected pyogenic spondylitis, tuberculous spondylitis, or metastasis were included. The procedure was performed on the XperGuide CBCT. Based on the initial CBCT, target points and entrance were determined, using dedicated guidance software (XperGuide), and the needle pathway was visualized in various reconstructed images. Needle aspiration was performed using Westcott needle and correct needle positioning was confirmed with the second CBCT. The technical success was defined as the needle tip reached within 5 mm of the target point. Culture, smear, and polymerase chain reaction of obtained samples were performed.
RESULTS
In all twelve patients, target areas could be determined based on XperCT data and achieved 100% technical success. Diagnosis could be made in 91.7% of cases and the median interventional procedure time was 27.8 minutes. There was no major complication in all patients.
CONCLUSION
Percutaneous needle aspiration of paraspinal lesions using XperGuide CBCT is easy, accurate, safe, and useful in determining the treatment of direction.
MeSH Terms
Figure
-
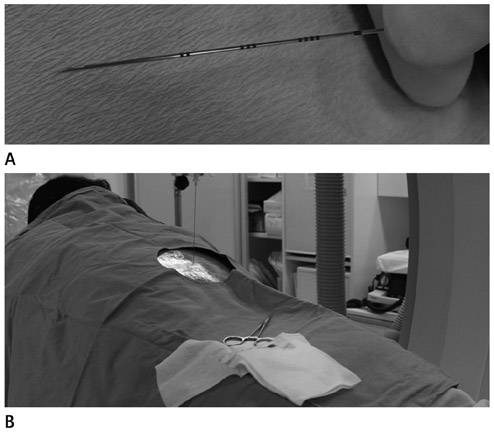
Fig. 1 Image-guided needle procedure. A. The Westcott needle has a beveled tip and a notched outer cannula. The side notch creates a second cutting edge and allows for aspiration of more material. B. The procedure was done with patient setting at prone position.
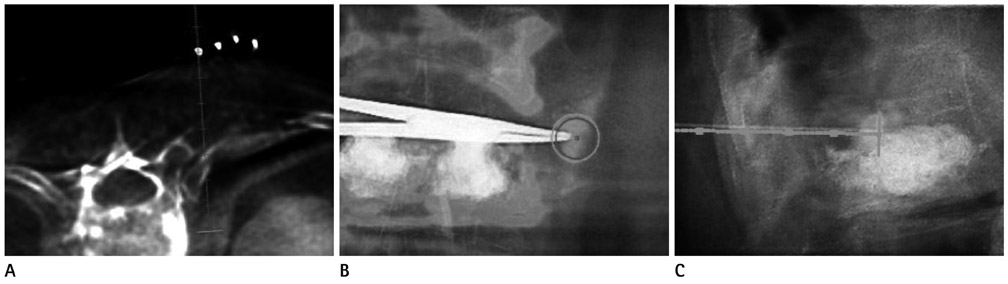
Fig. 2 A 69-year-old male, pyogenic spondylodiscitis. A. XperCT with axial needle progression view displays the planned needle trajectory in straight line. B. In the entry point view, entry and target points are displayed on overlaying images. C. Hybrid image overlaying the fluoroscopic image and the XperCT in the needle progression projection shows the biopsy needle advances along the planned trajectory, displayed as a straight line.
Cited by 1 articles
-
Musculoskeletal intervention
Jong Won Kwon
J Korean Med Assoc. 2015;58(6):502-515. doi: 10.5124/jkma.2015.58.6.502.
Reference
-
1. Kang M, Gupta S, Khandelwal N, Shankar S, Gulati M, Suri S. CT-guided fine-needle aspiration biopsy of spinal lesions. Acta Radiol. 1999. 40:474–478.2. Ozsarlak O, De Schepper AM, Wang X, De Raeve H. CT-guided percutaneous needle biopsy in spine lesions. JBR-BTR. 2003. 86:294–296.3. Kang KJ, Kim WH, Byun JS, Cho YK, Cho KJ, Moon KH, et al. Diagnostic usefulness of CT-guided percutaneous biopsy of the spine. J Korean Radiol Soc. 1999. 41:1195–1199.4. Siewerdsen JH, Moseley DJ, Burch S, Bisland SK, Bogaards A, Wilson BC, et al. Volume CT with a flat-panel detector on a mobile, isocentric C-arm: pre-clinical investigation in guidance of minimally invasive surgery. Med Phys. 2005. 32:241–254.5. Ritter D, Orman J, Schmidgunst C, Graumann R. 3D soft tissue imaging with a mobile C-arm. Comput Med Imaging Graph. 2007. 31:91–102.6. Braak SJ, van Strijen MJ, van Leersum M, van Es HW, van Heesewijk JP. Real-Time 3D fluoroscopy guidance during needle interventions: technique, accuracy, and feasibility. AJR Am J Roentgenol. 2010. 194:W445–W451.7. Leschka SC, Babic D, El Shikh S, Wossmann C, Schumacher M, Taschner CA. C-arm cone beam computed tomography needle path overlay for image-guided procedures of the spine and pelvis. Neuroradiology. 2012. 54:215–223.8. Rimondi E, Staals EL, Errani C, Bianchi G, Casadei R, Alberghini M, et al. Percutaneous CT-guided biopsy of the spine: results of 430 biopsies. Eur Spine J. 2008. 17:975–981.9. Nourbakhsh A, Grady JJ, Garges KJ. Percutaneous spine biopsy: a meta-analysis. J Bone Joint Surg Am. 2008. 90:1722–1725.10. Brenner DJ, Hall EJ. Computed tomography--an increasing source of radiation exposure. N Engl J Med. 2007. 357:2277–2284.11. Stoker J, Kipp JB, Geleijns K, van der Molen AJ, Venema HW. [Radiation exposure in computed tomography in the Netherlands: risk-benefit analysis]. Ned Tijdschr Geneeskd. 2009. 153:348–352.12. Braak SJ, van Strijen MJ, van Es HW, Nievelstein RA, van Heesewijk JP. Effective dose during needle interventions: cone-beam CT guidance compared with conventional CT guidance. J Vasc Interv Radiol. 2011. 22:455–461.13. Strocchi S, Colli V, Conte L. Multidetector CT fluoroscopy and cone-beam CT-guided percutaneous transthoracic biopsy: comparison based on patient doses. Radiat Prot Dosimetry. 2012. 151:162–165.14. Hwang CM, Shin MJ, Kim SM, Lee SH, Lee SM, Shin JH, et al. The diagnostic usefulness of CT-guided needle biopsy or aspiration in infectious spondylitis. J Korean Radiol Soc. 2003. 48:497–504.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Predicting Factors for Conversion from Fluoroscopy Guided Percutaneous Transthoracic Needle Biopsy to Cone-Beam CT Guided Percutaneous Transthoracic Needle Biopsy
- Three-dimensional imaging modalities in endodontics
- Experience of direct percutaneous sac injection in type II endoleak using cone beam computed tomography
- Percutaneous Fine Needle Aspiration Biopsy of Lung Masses
- Subcutaneous Seeding of Hepatoid Thymic Carcinoma after Percutaneous Needle Aspiration Biopsy
