Alveolar Soft Part Sarcoma: Clinical Presentation, Treatment and Outcome in a Series of 19 Patients
- Affiliations
-
- 1Department of Orthopaedic Surgery, Yonsei University College of Medicine, Seoul, Korea. choisidoru@yuhs.ac
- KMID: 1737635
- DOI: http://doi.org/10.4055/cios.2014.6.1.80
Abstract
- BACKGROUND
Alveolar soft part sarcoma (ASPS) is a rare soft tissue tumor that usually affects young patients. Because of the rarity of the disease, most reports relating to ASPS are in the form of case reports or small series.
METHODS
We performed a retrospective study to evaluate the clinicopathologic features, treatment, outcome and pattern of treatment failure in a consecutive series of patients with localized or metastatic ASPS between 1996 and 2011. Demographics, tumor sizes, sites and extent of disease, treatments provided, progression-free survival, and overall survival were evaluated.
RESULTS
A total of 19 patients were identified. The clinical assumptive diagnosis of the first medical examination doctor was benign soft tissue tumor in 5 cases (26%) and benign hemangioma in 4 cases (21%), delaying treatment. The most common location of primary tumor was the thigh. The median diameter of the mass was 55 mm (range, 10 to 130 mm). An R0 resection was obtained in 11 cases. Adjuvant radiotherapy was delivered in 8 cases; postoperative systemic chemotherapy was delivered in 10 cases. Eight out of 15 patients (53%) exhibited metastases either at presentation or later. Median overall follow-up was 54 months.
CONCLUSIONS
The treatment principle for alveolar soft tissue sarcoma is massive resection, and when the surgical margin is questionable, radiation treatment can be added for prevention of local recurrence. Also, due to discovery of metastases and local recurrence, even after 5 years of general treatment, outpatient department follow-up is needed, and we need to keep in mind that lung, intracranial, and bone metastases are common.
MeSH Terms
Figure
-
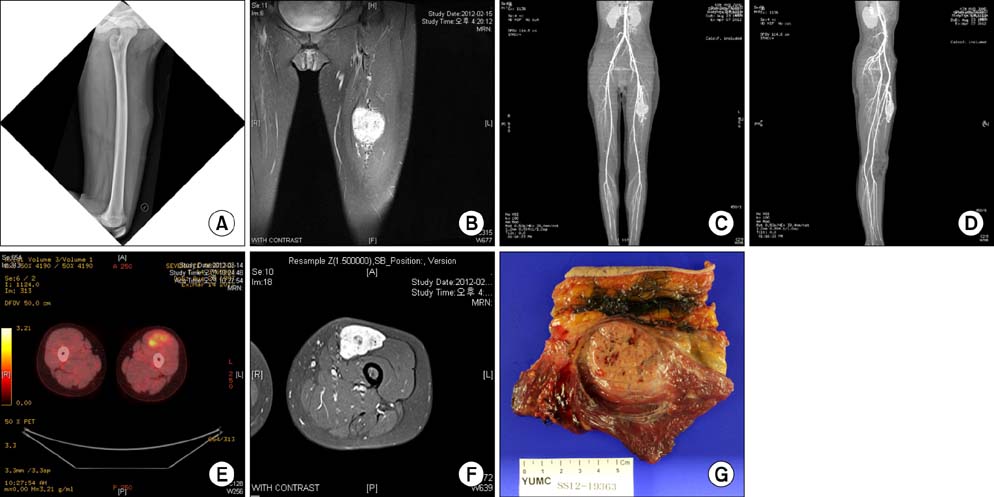
Fig. 1 A 14-year-old female patient presented with a chief complaint of growing palpable mass in the anterior aspect of the left mid thigh. (A) On the plain radiography of the left femur, soft tissue shadow was seen in the anterior aspect of the midshaft of the femur. (B) On T2-weighted coronal magnetic resonance image, there was a 7 × 5 × 3 mm-sized, well-enhanced soft tissue mass at the same site. (C,D) On computed tomography angiogram, a highly vascularized mass lesion was observed, and tortuous prominent blood vessels were seen on superior and inferior margins of the mass. (E,F) There was no metastasis seen on positron emission tomography computed tomography. (G) Incisional biopsy was performed and the mass was diagnosed as alveolar soft part sarcoma. A wide marginal excision was performed.
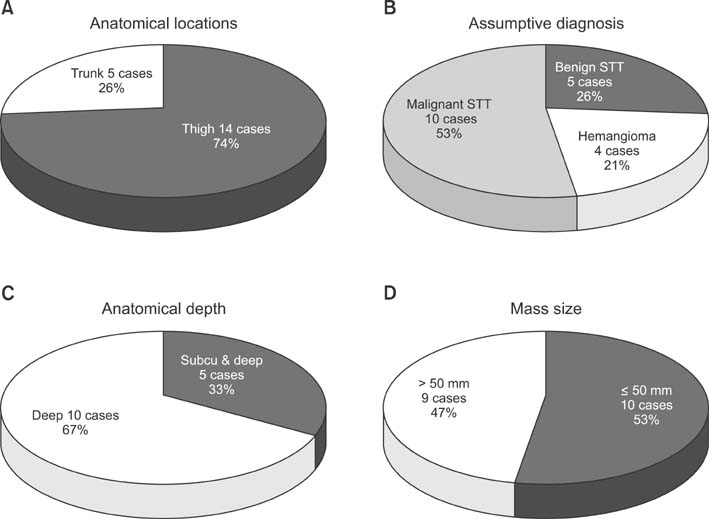
Fig. 2 (A) From a total of 19 cases, the mass was located in the trunk in 5 cases (26%) and thigh in 14 cases (74%). (B) During the first medical examination, benign soft tissue tumor was diagnosed in 5 cases (26%) and benign hemangioma in 4 cases (21%). (C) In the 15 cases in which magnetic resonance imaging was performed before the surgery, the mass was deep seated in 10 cases (67%) and located from subcutaneous layer to deep layer in 5 cases (33%). (D) Mass size exceeded 50 mm in 9 cases (47%), and it was less than or the same as that in 10 cases (53%). STT: soft tissue tumor.

Fig. 3 (A) Eight cases were transferred from other hospitals after surgery: unplanned excision in 6 cases and biopsy only in 2 cases. (B) Eight cases had metastases at the time of diagnosis: lung metastasis in 5 cases and multiple metastases in 3 cases (16%). (C) Among the cases with an operation at our hospital, the mass was classified as R0 in 11, R1 in 5, and R2 in 3. (D) In the 11 cases without metastases, lung metastasis was found in 2 and multiple metastases in another 2 during the outpatient follow-up. meta: metastasis.
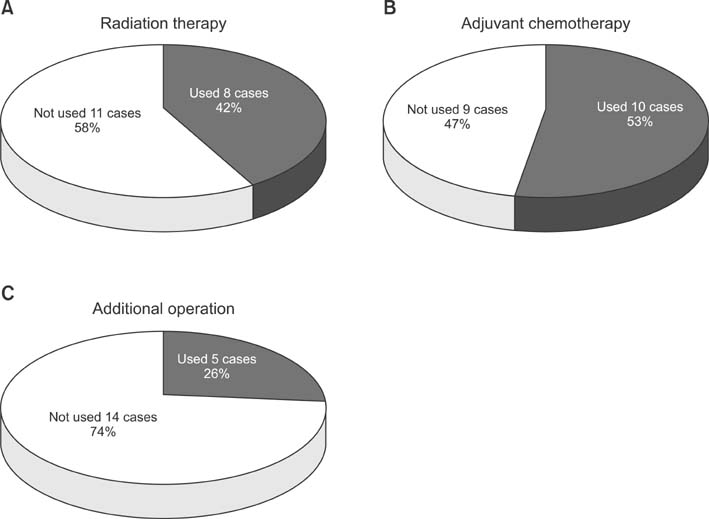
Fig. 4 (A) Eight cases (42%) had radiation therapy after operation. (B) Ten cases (53%) had adjuvant chemotherapy. (C) Five cases (26%) had an additional operation.
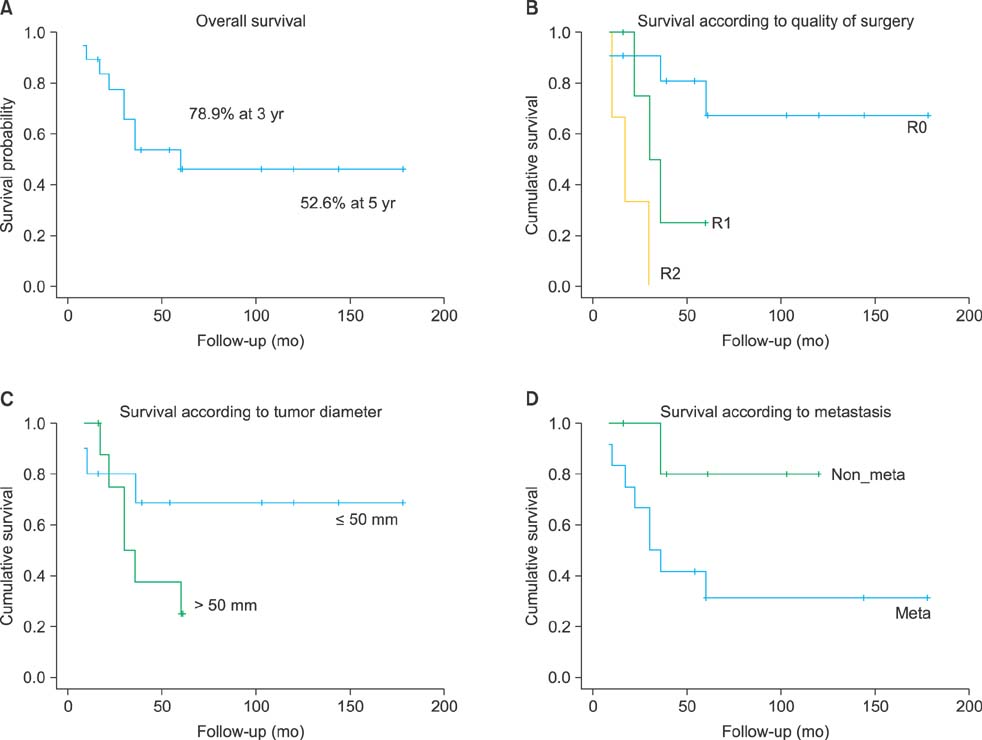
Fig. 5 (A) Overall 3-year survival rate was 78.9%. (B) The long-term survival rate was higher in R0 than R1 and R2 classified according to the quality of surgery. (C) The long-term survival rate was higher in patients with a tumor ≤ 50 mm in diameter than those with > 50 mm. (D) The long-term survival rate was higher in cases without metastases than in cases with metastases.
Reference
-
1. Christopherson WM, Foote FW Jr, Stewart FW. Alveolar soft-part sarcomas; structurally characteristic tumors of uncertain histogenesis. Cancer. 1952; 5(1):100–111.2. Ekfors TO, Kalimo H, Rantakokko V, Latvala M, Parvinen M. Alveolar soft part sarcoma: a report of two cases with some histochemical and ultrastructural observations. Cancer. 1979; 43(5):1672–1677.3. Lieberman PH, Brennan MF, Kimmel M, Erlandson RA, Garin-Chesa P, Flehinger BY. Alveolar soft-part sarcoma: a clinico-pathologic study of half a century. Cancer. 1989; 63(1):1–13.4. Fanburg-Smith JC, Miettinen M, Folpe AL, Weiss SW, Childers EL. Lingual alveolar soft part sarcoma; 14 cases: novel clinical and morphological observations. Histopathology. 2004; 45(5):526–537.5. Kayton ML. Alveolar soft part sarcoma. In : Enzinger FM, Weiss SW, editors. Soft tissue tumor. 3rd ed. St. Louis, MI: Mosby;1995. p. 1067–1074.6. Pang LM, Roebuck DJ, Griffith JF, Kumta SM, Metreweli C. Alveolar soft-part sarcoma: a rare soft-tissue malignancy with distinctive clinical and radiological features. Pediatr Radiol. 2001; 31(3):196–199.7. Iwamoto Y, Morimoto N, Chuman H, Shinohara N, Sugioka Y. The role of MR imaging in the diagnosis of alveolar soft part sarcoma: a report of 10 cases. Skeletal Radiol. 1995; 24(4):267–270.8. Suh JS, Cho J, Lee SH, et al. Alveolar soft part sarcoma: MR and angiographic findings. Skeletal Radiol. 2000; 29(12):680–689.9. Lorigan JG, O'Keeffe FN, Evans HL, Wallace S. The radiologic manifestations of alveolar soft-part sarcoma. AJR Am J Roentgenol. 1989; 153(2):335–339.10. Daigeler A, Kuhnen C, Hauser J, et al. Alveolar soft part sarcoma: clinicopathological findings in a series of 11 cases. World J Surg Oncol. 2008; 6:71.11. Günay C, Atalar H, Kaygusuz G, Yildiz Y, Saglik Y. Alveolar soft part sarcoma of the extremities: an evaluation of four cases. Acta Orthop Traumatol Turc. 2007; 41(4):326–331.12. Pennacchioli E, Fiore M, Collini P, et al. Alveolar soft part sarcoma: clinical presentation, treatment, and outcome in a series of 33 patients at a single institution. Ann Surg Oncol. 2010; 17(12):3229–3233.13. Ogose A, Yazawa Y, Ueda T, et al. Alveolar soft part sarcoma in Japan: multi-institutional study of 57 patients from the Japanese Musculoskeletal Oncology Group. Oncology. 2003; 65(1):7–13.14. Pisters PW, Leung DH, Woodruff J, Shi W, Brennan MF. Analysis of prognostic factors in 1,041 patients with localized soft tissue sarcomas of the extremities. J Clin Oncol. 1996; 14(5):1679–1689.15. Coindre JM, Terrier P, Bui NB, et al. Prognostic factors in adult patients with locally controlled soft tissue sarcoma: a study of 546 patients from the French Federation of Cancer Centers Sarcoma Group. J Clin Oncol. 1996; 14(3):869–877.16. Sherman N, Vavilala M, Pollock R, Romsdahl M, Jaffe N. Radiation therapy for alveolar soft-part sarcoma. Med Pediatr Oncol. 1994; 22(6):380–383.17. Pappo AS, Parham DM, Cain A, et al. Alveolar soft part sarcoma in children and adolescents: clinical features and outcome of 11 patients. Med Pediatr Oncol. 1996; 26(2):81–84.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Alveolar soft part Sarcoma with Metastasis to Bone: A Case Report
- Alveolar Soft-Part Sarcoma of the Female Genital Tract
- A Case of Alveolar Soft-Part Sarcoma
- Intracerebral Metastasis of Alveolar Soft Part Sarcoma: A case report and study on its histogenesis
- A Case of Alveolar Soft Part Sarcoma in the Orbit
