In Vivo Three-Dimensional Imaging Analysis of Femoral and Tibial Tunnel Locations in Single and Double Bundle Anterior Cruciate Ligament Reconstructions
- Affiliations
-
- 1Department of Orthopedic Surgery, Veterans Health Service Medical Center, Seoul, Korea.
- 2Department of Mechanical Engineering, Korea University, Seoul, Korea.
- 3Catholic Institute for Applied Anatomy, The Catholic University of Korea College of Medicine, Seoul, Korea.
- 4Department of Orthopedic Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. mdwang88@gmail.com
- KMID: 1737629
- DOI: http://doi.org/10.4055/cios.2014.6.1.32
Abstract
- BACKGROUND
Anatomic footprint restoration of anterior cruciate ligament (ACL) is recommended during reconstruction surgery. The purpose of this study was to compare and analyze the femoral and tibial tunnel positions of transtibial single bundle (SB) and transportal double bundle (DB) ACL reconstruction using three-dimensional computed tomography (3D-CT).
METHODS
In this study, 26 patients who underwent transtibial SB ACL reconstruction and 27 patients with transportal DB ACL reconstruction using hamstring autograft. 3D-CTs were taken within 1 week after the operation. The obtained digital images were then imported into the commercial package Geomagic Studio v10.0. The femoral tunnel positions were evaluated using the quadrant method. The mean, standard deviation, standard error, minimum, maximum, and 95% confidence interval values were determined for each measurement.
RESULTS
The femoral tunnel for the SB technique was located 35.07% +/- 5.33% in depth and 16.62% +/- 4.99% in height. The anteromedial (AM) and posterolateral (PL) tunnel of DB technique was located 30.48% +/- 5.02% in depth, 17.12% +/- 5.84% in height and 34.76% +/- 5.87% in depth, 45.55% +/- 6.88% in height, respectively. The tibial tunnel with the SB technique was located 45.43% +/- 4.81% from the anterior margin and 47.62% +/- 2.51% from the medial tibial articular margin. The AM and PL tunnel of the DB technique was located 33.76% +/- 7.83% from the anterior margin, 45.56% +/- 2.71% from the medial tibial articular margin and 53.19% +/- 3.74% from the anterior margin, 46.00% +/- 2.48% from the medial tibial articular margin, respectively. The tibial tunnel position with the transtibial SB technique was located between the AM and PL tunnel positions formed with the transportal DB technique.
CONCLUSIONS
Using the 3D-CT measuring method, the location of the tibia tunnel was between the AM and PL footprints, but the center of the femoral tunnel was at more shallow position from the AM bundle footprint when ACL reconstruction was performed by the transtibial SB technique.
MeSH Terms
Figure
-
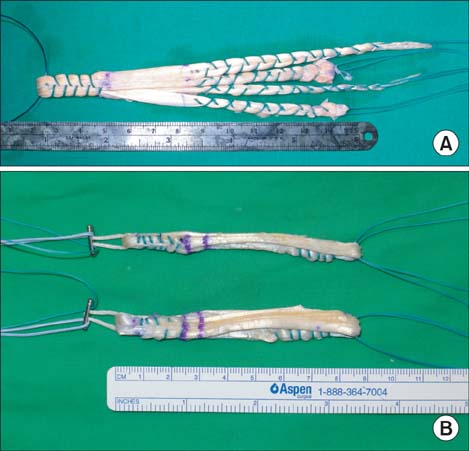
Fig. 1 (A) Double loop (four stranded) graft of hamstring tendon (semitendinosus and gracilis) was made for group I (transtibial single bundle technique). The double loop graft was composed of femoral side (30 mm), intraarticular portion (30 mm), and the rest for tibial tunnel including post-tie fixation. (B) A triple-stranded semitendinosus (for anteromedial bundle, bottom) and triple stranded gracilis (for posterolateral bundle, above), were made for group II (transportal double bundle technique). Each triple loop was composed of femoral side (25 mm), intraarticular portion (25 mm) and the rest for the tibia tunnel.
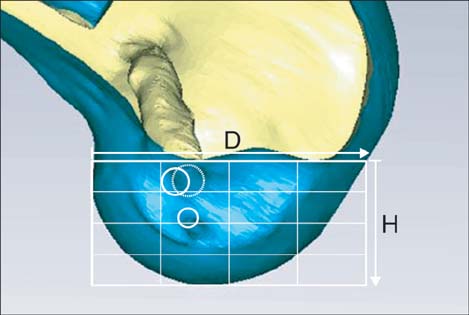
Fig. 2 A view of the lateral femoral condyle in a strictly lateral position, with both condyles superimposed, was obtained from the three-dimensional model using the Geomagic program. Distance D is defined as the total sagittal diameter of the lateral femoral condyle measured along the intercondylar notch roof. Distance H represents the height measured from the intercondylar notch roof to a line tangent to the distal subchondral contour of the condyle. The locations of the tunnels were quantified from the deepest subchondral contour to the center of the tunnel and were presented as the percentage distance from the intercondylar notch roof. The mean positions are expressed as a white dotted circle for the single bundle tunnel and white plane circles for the double bundle tunnels.
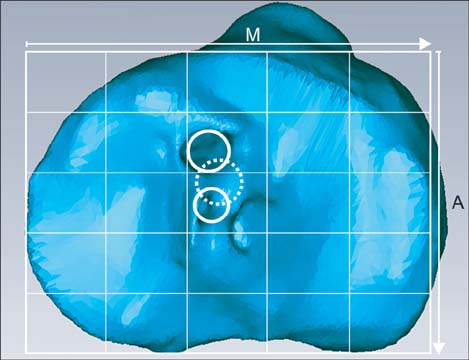
Fig. 3 The visual axis of the top view of the proximal tibia was perpendicular to the plane of the medial articular margin. A rectangular measurement frame was drawn with the posterior border tangent to the most posterior articular margins of both the medial and lateral tibial condyles. The anterior border of the rectangle was a line tangent to the most anterior articular margin of the medial tibial condyle. The tibial tunnel locations are expressed as percentages measured from the anterior border and the medial border from the total depth (A) and the total width (M) of the proximal tibia. The mean positions are expressed as dotted white circle for the single bundle tunnel and plain white circles for the double bundle tunnels.
Reference
-
1. Musahl V, Plakseychuk A, VanScyoc A, et al. Varying femoral tunnels between the anatomical footprint and isometric positions: effect on kinematics of the anterior cruciate ligament-reconstructed knee. Am J Sports Med. 2005; 33(5):712–718.2. Iriuchishima T, Tajima G, Ingham SJ, et al. Intercondylar roof impingement pressure after anterior cruciate ligament reconstruction in a porcine model. Knee Surg Sports Traumatol Arthrosc. 2009; 17(6):590–594.3. Kondo E, Yasuda K, Azuma H, Tanabe Y, Yagi T. Prospective clinical comparisons of anatomic double-bundle versus single-bundle anterior cruciate ligament reconstruction procedures in 328 consecutive patients. Am J Sports Med. 2008; 36(9):1675–1687.4. Hoser C, Tecklenburg K, Kuenzel KH, Fink C. Postoperative evaluation of femoral tunnel position in ACL reconstruction: plain radiography versus computed tomography. Knee Surg Sports Traumatol Arthrosc. 2005; 13(4):256–262.5. Basdekis G, Christel P, Anne F. Validation of the position of the femoral tunnels in anatomic double-bundle ACL reconstruction with 3-D CT scan. Knee Surg Sports Traumatol Arthrosc. 2009; 17(9):1089–1094.6. Lertwanich P, Martins CA, Asai S, Ingham SJ, Smolinski P, Fu FH. Anterior cruciate ligament tunnel position measurement reliability on 3-dimensional reconstructed computed tomography. Arthroscopy. 2011; 27(3):391–398.7. Forsythe B, Kopf S, Wong AK, et al. The location of femoral and tibial tunnels in anatomic double-bundle anterior cruciate ligament reconstruction analyzed by three-dimensional computed tomography models. J Bone Joint Surg Am. 2010; 92(6):1418–1426.8. Ahn JH, Lee YS, Ha HC. Anterior cruciate ligament reconstruction with preservation of remnant bundle using hamstring autograft: technical note. Arch Orthop Trauma Surg. 2009; 129(8):1011–1015.9. Hantes ME, Mastrokalos DS, Yu J, Paessler HH. The effect of early motion on tibial tunnel widening after anterior cruciate ligament replacement using hamstring tendon grafts. Arthroscopy. 2004; 20(6):572–580.10. Ahn JH, Park JS, Lee YS, Cho YJ. Femoral bioabsorbable cross-pin fixation in anterior cruciate ligament reconstruction. Arthroscopy. 2007; 23(10):1093–1099.11. Ferretti M, Ekdahl M, Shen W, Fu FH. Osseous landmarks of the femoral attachment of the anterior cruciate ligament: an anatomic study. Arthroscopy. 2007; 23(11):1218–1225.12. Bernard M, Hertel P, Hornung H, Cierpinski T. Femoral insertion of the ACL: radiographic quadrant method. Am J Knee Surg. 1997; 10(1):14–21.13. Amis AA, Beynnon B, Blankevoort L, et al. Proceedings of the ESSKA scientific workshop on reconstruction of the anterior and posterior cruciate ligaments. Knee Surg Sports Traumatol Arthrosc. 1994; 2(3):124–132.14. Lysholm J, Gillquist J. Evaluation of knee ligament surgery results with special emphasis on use of a scoring scale. Am J Sports Med. 1982; 10(3):150–154.15. Tegner Y, Lysholm J. Rating systems in the evaluation of knee ligament injuries. Clin Orthop Relat Res. 1985; (198):43–49.16. Hefti F, Muller W, Jakob RP, Staubli HU. Evaluation of knee ligament injuries with the IKDC form. Knee Surg Sports Traumatol Arthrosc. 1993; 1(3-4):226–234.17. Ho JY, Gardiner A, Shah V, Steiner ME. Equal kinematics between central anatomic single-bundle and double-bundle anterior cruciate ligament reconstructions. Arthroscopy. 2009; 25(5):464–472.18. Zantop T, Diermann N, Schumacher T, Schanz S, Fu FH, Petersen W. Anatomical and nonanatomical double-bundle anterior cruciate ligament reconstruction: importance of femoral tunnel location on knee kinematics. Am J Sports Med. 2008; 36(4):678–685.19. Aglietti P, Zaccherotti G, Menchetti PP, De Biase P. A comparison of clinical and radiological parameters with two arthroscopic techniques for anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 1995; 3(1):2–8.20. Edwards A, Bull AM, Amis AA. The attachments of the anteromedial and posterolateral fibre bundles of the anterior cruciate ligament. Part 2: femoral attachment. Knee Surg Sports Traumatol Arthrosc. 2008; 16(1):29–36.21. Harner CD, Marks PH, Fu FH, Irrgang JJ, Silby MB, Mengato R. Anterior cruciate ligament reconstruction: endoscopic versus two-incision technique. Arthroscopy. 1994; 10(5):502–512.22. Amis AA, Jakob RP. Anterior cruciate ligament graft positioning, tensioning and twisting. Knee Surg Sports Traumatol Arthrosc. 1998; 6:Suppl 1. S2–S12.23. Zantop T, Wellmann M, Fu FH, Petersen W. Tunnel positioning of anteromedial and posterolateral bundles in anatomic anterior cruciate ligament reconstruction: anatomic and radiographic findings. Am J Sports Med. 2008; 36(1):65–72.24. Tsukada H, Ishibashi Y, Tsuda E, Fukuda A, Toh S. Anatomical analysis of the anterior cruciate ligament femoral and tibial footprints. J Orthop Sci. 2008; 13(2):122–129.25. Inoue M, Tokuyasu S, Kuwahara S, et al. Tunnel location in transparent 3-dimensional CT in anatomic double-bundle anterior cruciate ligament reconstruction with the trans-tibial tunnel technique. Knee Surg Sports Traumatol Arthrosc. 2010; 18(9):1176–1183.26. Farrow LD, Gillespie RJ, Victoroff BN, Cooperman DR. Radiographic location of the lateral intercondylar ridge: its relationship to Blumensaat's line. Am J Sports Med. 2008; 36(10):2002–2006.27. Gavriilidis I, Motsis EK, Pakos EE, Georgoulis AD, Mitsionis G, Xenakis TA. Transtibial versus anteromedial portal of the femoral tunnel in ACL reconstruction: a cadaveric study. Knee. 2008; 15(5):364–367.28. Dargel J, Schmidt-Wiethoff R, Fischer S, Mader K, Koebke J, Schneider T. Femoral bone tunnel placement using the transtibial tunnel or the anteromedial portal in ACL reconstruction: a radiographic evaluation. Knee Surg Sports Traumatol Arthrosc. 2009; 17(3):220–227.29. Giron F, Cuomo P, Edwards A, Bull AM, Amis AA, Aglietti P. Double-bundle "anatomic" anterior cruciate ligament reconstruction: a cadaveric study of tunnel positioning with a transtibial technique. Arthroscopy. 2007; 23(1):7–13.30. Bedi A, Musahl V, Steuber V, et al. Transtibial versus anteromedial portal reaming in anterior cruciate ligament reconstruction: an anatomic and biomechanical evaluation of surgical technique. Arthroscopy. 2011; 27(3):380–390.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Single Bundle Anterior Cruciate Ligament Reconstruction
- The Correlation of Tunnel Position, Orientation and Tunnel Enlargement in Outside-in Single-Bundle Anterior Cruciate Ligament Reconstruction
- Three-Dimensional Reconstruction Computed Tomography Evaluation of Tunnel Location during Single-Bundle Anterior Cruciate Ligament Reconstruction: A Comparison of Transtibial and 2-Incision Tibial Tunnel-Independent Techniques
- Three-Dimensional Reconstruction Computed Tomography Evaluation of the Tunnel Location and Angle in Anatomic Single-Bundle Anterior Cruciate Ligament Reconstruction: A Comparison of the Anteromedial Portal and Outside-in Techniques
- Kinematic Analysis of Five Different Anterior Cruciate Ligament Reconstruction Techniques
