Three-Dimensional Reconstruction Computed Tomography Evaluation of Tunnel Location during Single-Bundle Anterior Cruciate Ligament Reconstruction: A Comparison of Transtibial and 2-Incision Tibial Tunnel-Independent Techniques
- Affiliations
-
- 1Department of Orthopedic Surgery, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea. kneedoc@naver.com
- KMID: 1402323
- DOI: http://doi.org/10.4055/cios.2013.5.1.26
Abstract
- BACKGROUND
Anatomic tunnel positioning is important in anterior cruciate ligament (ACL) reconstructive surgery. Recent studies have suggested the limitations of a traditional transtibial technique to place the ACL graft within the anatomic tunnel position of the ACL on the femur. The purpose of this study is to determine if the 2-incision tibial tunnel-independent technique can place femoral tunnel to native ACL center when compared with the transtibial technique, as the placement with the tibial tunnel-independent technique is unconstrained by tibial tunnel.
METHODS
In sixty-nine patients, single-bundle ACL reconstruction with preservation of remnant bundle using hamstring tendon autograft was performed. Femoral tunnel locations were measured with quadrant methods on the medial to lateral view of the lateral femoral condyle. Tibial tunnel locations were measured in the anatomical coordinates axis on the top view of the proximal tibia. These measurements were compared with reference data on anatomical tunnel position.
RESULTS
With the quadrant method, the femoral tunnel centers of the transtibial technique and tibial tunnel-independent technique were located. The mean (+/- standard deviation) was 36.49% +/- 7.65% and 24.71% +/- 4.90%, respectively, from the over-the-top, along the notch roof (parallel to the Blumensaat line); and at 7.71% +/- 7.25% and 27.08% +/- 7.05%, from the notch roof (perpendicular to the Blumensaat line). The tibial tunnel centers of the transtibial technique and tibial tunnel-independent technique were located at 39.83% +/- 8.20% and 36.32% +/- 8.10%, respectively, of the anterior to posterior tibial plateau depth; and at 49.13% +/- 4.02% and 47.75% +/- 4.04%, of the medial to lateral tibial plateau width. There was no statistical difference between the two techniques in tibial tunnel position. The tibial tunnel-independent technique used in this study placed femoral tunnel closer to the anatomical ACL anteromedial bundle center. In contrast, the transtibial technique placed the femoral tunnel more shallow and higher from the anatomical position, resulting in more vertical grafts.
CONCLUSIONS
After single-bundle ACL reconstruction, three-dimensional computed tomography showed that the tibial tunnel-independent technique allows for the placement of the graft closer to the anatomical femoral tunnel position when compared with the traditional transtibial technique.
Keyword
MeSH Terms
Figure
-
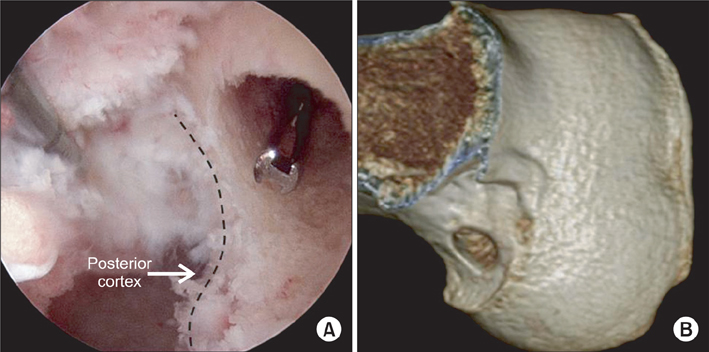
Fig. 1 Femoral tunnel made by the transtibial technique. (A) The femoral tunnel was made 1 to 2 mm before the posterior cortex. (B) Three-dimensional computed tomography shows the femoral tunnel made by the transtibial technique.
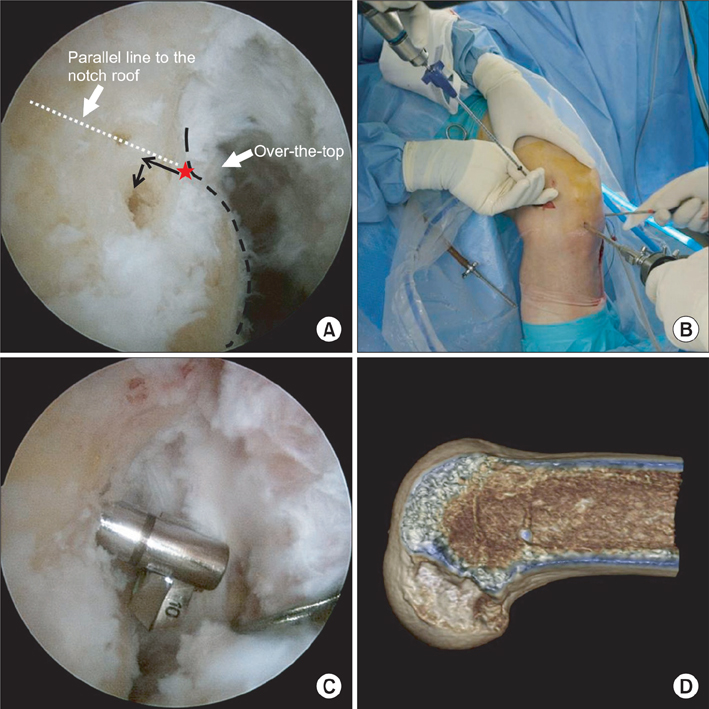
Fig. 2 Femoral tunnel made by the tibial tunnel-independent technique. (A) The marking hole was located at 5 to 6 mm shallow from the most proximal high deep point on the cartilage-bone border of lateral condyle (over-the-top), and from this point, 2 to 3 mm low. (B) Through a stab incision at the distal midlateral femoral metaphyseal flare, 3.5 mm outside-in minimally invasive drilling pin (Flipcutter) was introduced. (C) The cutter chosen to match the diameter of the graft; 10 mm drilled to create an outside-in femoral tunnel. (D) Three-dimensional computed tomography shows the femoral tunnel made by the tibial tunnel-independent technique.
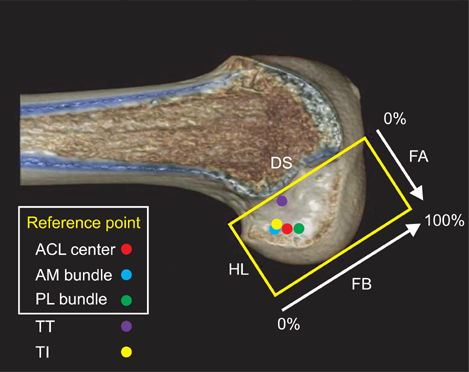
Fig. 3 On the lateral femoral side of three-dimensional computed tomography, the location of the transtibial and tibial independent femoral tunnel are shown. The location of tunnel was quantified from center of the tunnel to the deepest subchondral bone contour (distance FA) and the intercondylar notch roof (distance FB). ACL: anterior cruciate ligament, AM: anteromedial, PL: posterolateral, TT: transtibial, TI: tibial tunnel-independent, DS: distance deep to shallow, HL: distance high to low, FA: femur 'A' line, FB: femur 'B' line.
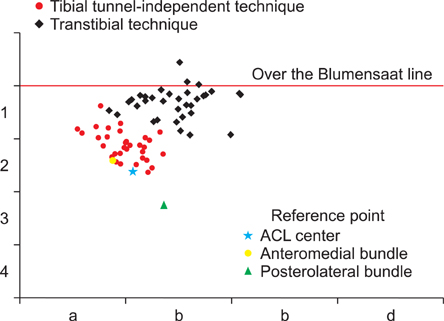
Fig. 4 4 × 4 grid of quadrant method, by tibial tunnel-independent technique: 9 (25.7%) and 14 (40.0%) of 35 femoral tunnels located in 2a and 2b grid, respectively. On the other hand, by transtibial technique, 28 (82.4%) of 34 femoral tunnels were located in 1b grid; furthermore, 3 of 34 were located over the Blumensaat line (red line).

Fig. 5 On the top view of the proximal tibia, the location of the transtibial and tibial independent tibial tunnel are shown. The location of tunnel was measured from the anterior border (distance TA) and medial border (distance TB). AP: distance anterior to posterior, ML: distance medial to lateral, AM: anteromedial, PL: posterolateral, TT: transtibial, TI: tibial tunnel-independent, TA: tibia 'A' line, TB: tibia 'B' line.
Reference
-
1. Asagumo H, Kimura M, Kobayashi Y, Taki M, Takagishi K. Anatomic reconstruction of the anterior cruciate ligament using double-bundle hamstring tendons: surgical techniques, clinical outcomes, and complications. Arthroscopy. 2007. 23(6):602–609.
Article2. Heming JF, Rand J, Steiner ME. Anatomical limitations of transtibial drilling in anterior cruciate ligament reconstruction. Am J Sports Med. 2007. 35(10):1708–1715.
Article3. Getelman MH, Friedman MJ. Revision anterior cruciate ligament reconstruction surgery. J Am Acad Orthop Surg. 1999. 7(3):189–198.
Article4. Piasecki DP, Bach BR Jr, Espinoza Orias AA, Verma NN. Anterior cruciate ligament reconstruction: can anatomic femoral placement be achieved with a transtibial technique? Am J Sports Med. 2011. 39(6):1306–1315.5. Steiner ME, Battaglia TC, Heming JF, Rand JD, Festa A, Baria M. Independent drilling outperforms conventional transtibial drilling in anterior cruciate ligament reconstruction. Am J Sports Med. 2009. 37(10):1912–1919.
Article6. Cain EL Jr, Clancy WG Jr. Anatomic endoscopic anterior cruciate ligament reconstruction with patella tendon autograft. Orthop Clin North Am. 2002. 33(4):717–725.
Article7. Scopp JM, Jasper LE, Belkoff SM, Moorman CT 3rd. The effect of oblique femoral tunnel placement on rotational constraint of the knee reconstructed using patellar tendon autografts. Arthroscopy. 2004. 20(3):294–299.
Article8. Brophy RH, Pearle AD. Single-bundle anterior cruciate ligament reconstruction: a comparison of conventional, central, and horizontal single-bundle virtual graft positions. Am J Sports Med. 2009. 37(7):1317–1323.
Article9. Arnold MP, Kooloos J, van Kampen A. Single-incision technique misses the anatomical femoral anterior cruciate ligament insertion: a cadaver study. Knee Surg Sports Traumatol Arthrosc. 2001. 9(4):194–199.
Article10. Tsukada H, Ishibashi Y, Tsuda E, Fukuda A, Toh S. Anatomical analysis of the anterior cruciate ligament femoral and tibial footprints. J Orthop Sci. 2008. 13(2):122–129.
Article11. Forsythe B, Kopf S, Wong AK, et al. The location of femoral and tibial tunnels in anatomic double-bundle anterior cruciate ligament reconstruction analyzed by three-dimensional computed tomography models. J Bone Joint Surg Am. 2010. 92(6):1418–1426.
Article12. Bedi A, Altchek DW. The "footprint" anterior cruciate ligament technique: an anatomic approach to anterior cruciate ligament reconstruction. Arthroscopy. 2009. 25(10):1128–1138.
Article13. Amis AA, Beynnon B, Blankevoort L, et al. Proceedings of the ESSKA Scientific Workshop on Reconstruction of the Anterior and Posterior Cruciate Ligaments. Knee Surg Sports Traumatol Arthrosc. 1994. 2(3):124–132.
Article14. Kaseta MK, DeFrate LE, Charnock BL, Sullivan RT, Garrett WE Jr. Reconstruction technique affects femoral tunnel placement in ACL reconstruction. Clin Orthop Relat Res. 2008. 466(6):1467–1474.
Article15. Howell SM, Gittins ME, Gottlieb JE, Traina SM, Zoellner TM. The relationship between the angle of the tibial tunnel in the coronal plane and loss of flexion and anterior laxity after anterior cruciate ligament reconstruction. Am J Sports Med. 2001. 29(5):567–574.
Article16. Howell SM, Deutsch ML. Comparison of endoscopic and two-incision techniques for reconstructing a torn anterior cruciate ligament using hamstring tendons. Arthroscopy. 1999. 15(6):594–606.
Article17. Kondo E, Yasuda K, Ichiyama H, Azuma C, Tohyama H. Radiologic evaluation of femoral and tibial tunnels created with the transtibial tunnel technique for anatomic double-bundle anterior cruciate ligament reconstruction. Arthroscopy. 2007. 23(8):869–876.
Article18. Kopf S, Forsythe B, Wong AK, et al. Nonanatomic tunnel position in traditional transtibial single-bundle anterior cruciate ligament reconstruction evaluated by three-dimensional computed tomography. J Bone Joint Surg Am. 2010. 92(6):1427–1431.
Article19. Behrendt S, Richter J. Anterior cruciate ligament reconstruction: drilling a femoral posterolateral tunnel cannot be accomplished using an over-the-top step-off drill guide. Knee Surg Sports Traumatol Arthrosc. 2010. 18(9):1252–1256.
Article20. Abebe ES, Moorman CT 3rd, Dziedzic TS, et al. Femoral tunnel placement during anterior cruciate ligament reconstruction: an in vivo imaging analysis comparing transtibial and 2-incision tibial tunnel-independent techniques. Am J Sports Med. 2009. 37(10):1904–1911.
Article21. Harner CD, Honkamp NJ, Ranawat AS. Anteromedial portal technique for creating the anterior cruciate ligament femoral tunnel. Arthroscopy. 2008. 24(1):113–115.
Article22. Hantes ME, Zachos VC, Liantsis A, Venouziou A, Karantanas AH, Malizos KN. Differences in graft orientation using the transtibial and anteromedial portal technique in anterior cruciate ligament reconstruction: a magnetic resonance imaging study. Knee Surg Sports Traumatol Arthrosc. 2009. 17(8):880–886.
Article23. Anderson AF, Snyder RB, Lipscomb AB Jr. Anterior cruciate ligament reconstruction: a prospective randomized study of three surgical methods. Am J Sports Med. 2001. 29(3):272–279.24. Fujita N, Kuroda R, Matsumoto T, et al. Comparison of the clinical outcome of double-bundle, anteromedial single-bundle, and posterolateral single-bundle anterior cruciate ligament reconstruction using hamstring tendon graft with minimum 2-year follow-up. Arthroscopy. 2011. 27(7):906–913.
Article25. Kato Y, Maeyama A, Lertwanich P, et al. Biomechanical comparison of different graft positions for single-bundle anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2012. 03. 15. http://dx.doi.org/10.1007/s00167-012-1951-4.
Article26. Lertwanich P, Martins CA, Asai S, Ingham SJ, Smolinski P, Fu FH. Anterior cruciate ligament tunnel position measurement reliability on 3-dimensional reconstructed computed tomography. Arthroscopy. 2011. 27(3):391–398.
Article27. Zantop T, Petersen W. Double bundle revision of a malplaced single bundle vertical ACL reconstruction: ACL revision surgery using a two femoral tunnel technique. Arch Orthop Trauma Surg. 2008. 128(11):1287–1294.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Femoral Tunnel Drilling Techniques in Anterior Cruciate Ligament Reconstruction
- Single Bundle Anterior Cruciate Ligament Reconstruction
- Tomographic Study of Femoral Positioning in Anterior Cruciate Ligament Reconstruction Using the Transtibial Technique
- The Correlation of Tunnel Position, Orientation and Tunnel Enlargement in Outside-in Single-Bundle Anterior Cruciate Ligament Reconstruction
- Three-Dimensional Reconstruction Computed Tomography Evaluation of the Tunnel Location and Angle in Anatomic Single-Bundle Anterior Cruciate Ligament Reconstruction: A Comparison of the Anteromedial Portal and Outside-in Techniques
