Image Quality and Radiation Dose of Lower Extremity CT Angiography in 128 Slice Dual-Source CT: Comparison of High Pitch and Low Pitch
- Affiliations
-
- 1Department of Radiology, Research Institute for Convergence of Biomedical Science and Technology, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Yangsan, Korea. kschoo0618@naver.com
- 2Department of Radiology, Pusan National University Hospital, Pusan National University School of Medicine, Busan, Korea.
- 3Department of Family Medicine, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Yangsan, Korea.
- 4Department of Cardiology, Gim Hae Jungang Hospital, Gimhae, Korea.
- KMID: 1736477
- DOI: http://doi.org/10.3348/jksr.2014.71.3.128
Abstract
- PURPOSE
The objective of this study is to compare image quality and radiation dose of high pitch (3) CT angiography (CTA) with 128-slice dual-source CT in lower extremity arteries with that of low pitch (0.6) CTA.
MATERIALS AND METHODS
A total of 136 patients were divided into two groups; high pitch (3) group included 67 patients and low pitch (0.6) group included 69 patients. For quantitative analysis, we calculated the mean arterial attenuation, mean coefficient variation of arterial attenuations, mean contrast-to-noise ratio, mean figure of merit (FOM), and mean standard deviation of CT density of muscle. In addition, visual scores were used for qualitative evaluation, and radiation doses were reported in the two groups.
RESULTS
The mean dose-length product was decreased by 31% at high pitch (409.49 +/- 37.71 mGy.cm vs. 592.98 +/- 59.69 mGy.cm), and the mean volume CT dose index was also significantly decreased at high pitch (2.91 +/- 0.14 mGy vs. 4.70 +/- 0.30 mGy). However, other quantitative analysis showed no significant intergroup differences, except in mean FOM. Visual scores showed no significant intergroup difference.
CONCLUSION
Despite changing the pitch from 0.6 to 3, the image quality of CTA was not degraded and radiation dose was reduced by 31%.
MeSH Terms
Figure
-
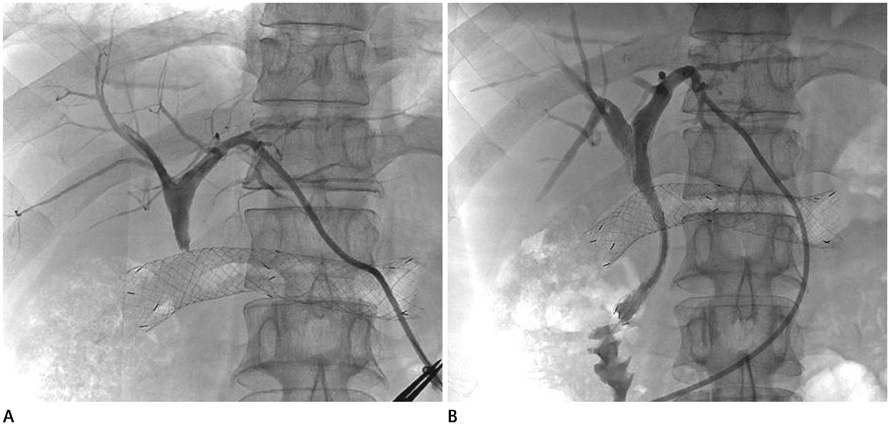
Fig. 1 A 50-year-old male with pyloric cancer. A. Obstructive jaundice developed 5 days after placement of a pyloric stent. Tubogram after percutaneous biliary drainage shows no passage of contrast media at the common bile duct level. B. The follow-up tubogram 3 days after placement of the biliary stent shows good passage of contrast media into the duodenum.
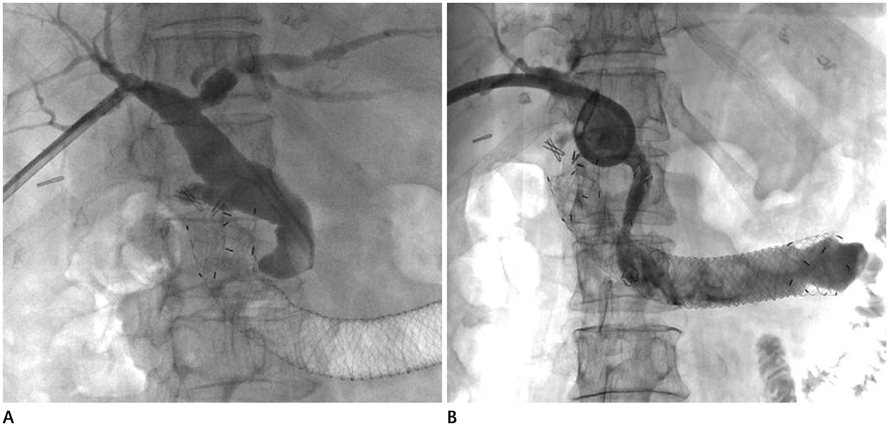
Fig. 2 A 76-year-old female with a duodenal carcinoma in the second and third portion of the duodenum. A. Obstructive jaundice developed 6 days after placement of a duodenal stent. Tubogram after percutaneous biliary drainage shows complete occlusion of the biliary system at the Ampulla of Vater level. B. Follow-up tubogram 3 days after placement of the biliary stent shows good contrast media passage into the duodenum and jejunum through the biliary and duodenal stents.
Reference
-
1. Bessoud B, de Baere T, Denys A, Kuoch V, Ducreux M, Precetti S, et al. Malignant gastroduodenal obstruction: palliation with self-expanding metallic stents. J Vasc Interv Radiol. 2005; 16(2 Pt 1):247–253.2. Jung GS, Song HY, Seo TS, Park SJ, Koo JY, Huh JD, et al. Malignant gastric outlet obstructions: treatment by means of coaxial placement of uncovered and covered expandable nitinol stents. J Vasc Interv Radiol. 2002; 13:275–283.3. Dormann A, Meisner S, Verin N, Wenk Lang A. Self-expanding metal stents for gastroduodenal malignancies: systematic review of their clinical effectiveness. Endoscopy. 2004; 36:543–550.4. van Hooft J, Mutignani M, Repici A, Messmann H, Neuhaus H, Fockens P. First data on the palliative treatment of patients with malignant gastric outlet obstruction using the WallFlex enteral stent: a retrospective multicenter study. Endoscopy. 2007; 39:434–439.5. Baron TH, Harewood GC. Enteral self-expandable stents. Gastrointest Endosc. 2003; 58:421–433.6. Gutzeit A, Binkert CA, Schoch E, Sautter T, Jost R, Zollikofer CL. Malignant gastroduodenal obstruction: treatment with self-expanding uncovered wallstent. Cardiovasc Intervent Radiol. 2009; 32:97–105.7. Kim KO, Kim TN, Lee HC. Effectiveness of combined biliary and duodenal stenting in patients with malignant biliary and duodenal obstruction. Scand J Gastroenterol. 2012; 47:962–967.8. Adler DG, Baron TH. Endoscopic palliation of malignant gastric outlet obstruction using self-expanding metal stents: experience in 36 patients. Am J Gastroenterol. 2002; 97:72–78.9. Yates MR 3rd, Morgan DE, Baron TH. Palliation of malignant gastric and small intestinal strictures with self-expandable metal stents. Endoscopy. 1998; 30:266–272.10. Profili S, Meloni GB, Bifulco V, Conti M, Feo CF, Canalis GC. Self-expandable metal stents in the treatment of antro-pyloric and/or duodenal strictures. Acta Radiol. 2001; 42:176–180.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Image Quality and Radiation Dose of High-Pitch Dual-Source Spiral Cardiothoracic Computed Tomography in Young Children with Congenital Heart Disease: Comparison of Non-Electrocardiography Synchronization and Prospective Electrocardiography Triggering
- Prospectively Electrocardiogram-Gated High-Pitch Spiral Acquisition Mode Dual-Source CT Coronary Angiography in Patients with High Heart Rates: Comparison with Retrospective Electrocardiogram-Gated Spiral Acquisition Mode
- Evaluation of the effective dose and image quality of low-dose multi-detector CT for orthodontic treatment planning
- Comparison of Radiation Dose and Image Quality between the 2nd Generation and 3rd Generation Dual-Source Single-Energy and Dual-Source Dual-Energy CT of the Abdomen
- Technical Aspect of Coronary CT Angiography: Imaging Tips and Safety Issues
