Treatment of Malignant Biliary Obstruction with a PTFE-Covered Self-Expandable Nitinol Stent
- Affiliations
-
- 1Department of Radiology, Chonbuk National University Medical School and Hospital, Chonju, Korea. ymhan@chonbuk.ac.kr
- 2Institute of Cardiovascular Research, Chonbuk National University Medical School and Hospital, Chonju, Korea.
- 3Department of Internal Medicine, Chonbuk National University Medical School and Hospital, Chonju, Korea.
- KMID: 1734290
- DOI: http://doi.org/10.3348/kjr.2007.8.5.410
Abstract
OBJECTIVE
We wanted to determine the technical and clinical efficacy of using a PTFE-covered self-expandable nitinol stent for the palliative treatment of malignant biliary obstruction. MATERIALS AND METHODS: Thirty-seven patients with common bile duct strictures caused by malignant disease were treated by placing a total of 37 nitinol PTFE stents. These stents were covered with PTFE with the exception of the last 5 mm at each end; the stent had an unconstrained diameter of 10 mm and a total length of 50-80 mm. The patient survival rate and stent patency rate were calculated by performing Kaplan-Meier survival analysis. The bilirubin, serum amylase and lipase levels before and after stent placement were measured and then compared using a Wilcoxon signed-rank test. The average follow-up duration was 27.9 weeks (range: 2-81 weeks). RESULTS: Placement was successful in all cases. Seventy-six percent of the patients (28/37) experienced adequate palliative drainage for the remainder of their lives. There were no immediate complications. Three patients demonstrated stent sludge occlusion that required PTBD (percutaneous transhepatic biliary drainage) irrigation. Two patients experienced delayed stent migration with stone formation at 7 and 27 weeks of follow-up, respectively. Stent insertion resulted in acute elevations of the amylase and lipase levels one day after stent insertion in 11 patients in spite of performing endoscopic sphincterotomy (4/6). The bilirubin levels were significantly reduced one week after stent insertion (p < 0.01). The 30-day mortality rate was 8% (3/37), and the survival rates were 49% and 27% at 20 and 50 weeks, respectively. The primary stent patency rates were 85%, and 78% at 20 and 50 weeks, respectively. CONCLUSION: The PTFE-covered self-expandable nitinol stent is safe to use with acceptable complication rates. This study is similar to the previous studies with regard to comparing the patency rates and survival rates.
Keyword
MeSH Terms
-
Adenocarcinoma/*complications
Aged
Aged, 80 and over
Alloys/adverse effects/*therapeutic use
Cholestasis, Extrahepatic/etiology/*surgery
Coated Materials, Biocompatible/*therapeutic use
Common Bile Duct/radiography/surgery
Digestive System Neoplasms/*complications
Equipment Design
Female
Follow-Up Studies
Humans
Male
Middle Aged
Palliative Care/methods
Pilot Projects
Polytetrafluoroethylene/adverse effects/*therapeutic use
Postoperative Complications/diagnosis/epidemiology
Prospective Studies
*Stents/adverse effects
Survival Analysis
Treatment Outcome
Figure
-
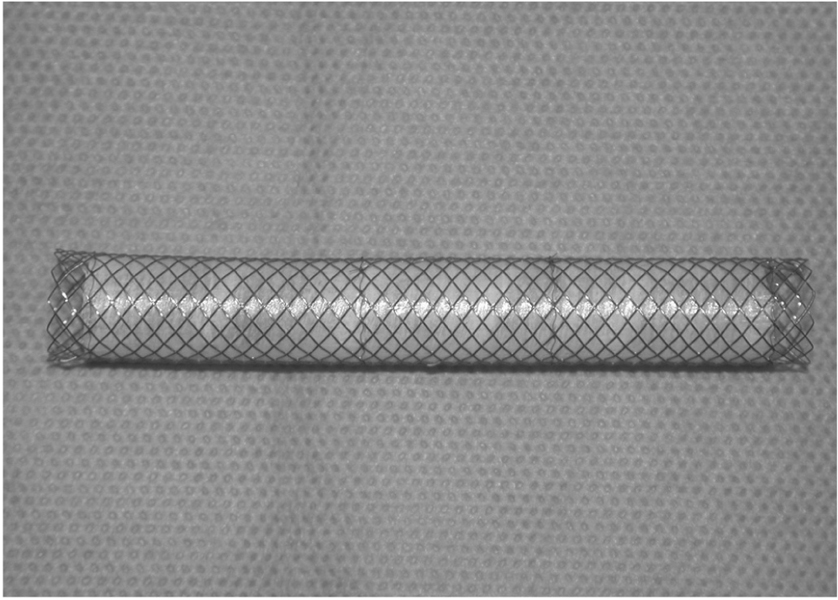
Fig. 1 The PTFE-covered self-expanding Niti-S stent endoprosthesis. The stent is a woven, monofilament structure composed of nitinol, and it is covered on its interior surface by PTFE.
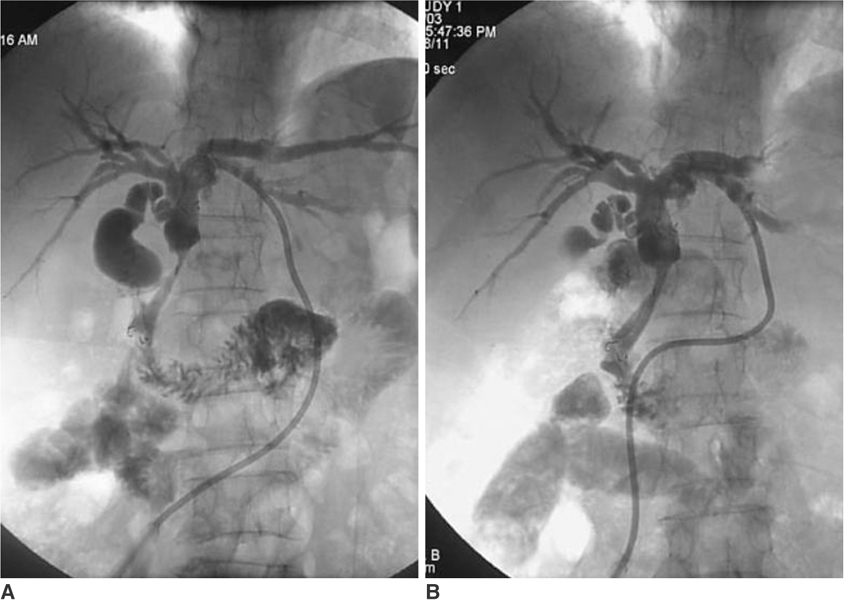
Fig. 2 A 68-year-old female with common bile duct carcinoma. A. The tubogram taken immediately after stent insertion shows good stent patency and correct positioning. B. This one-week follow-up tubogram shows good stent function. The distance between the end of the stent and the bifurcation of the common hepatic duct shows no change.
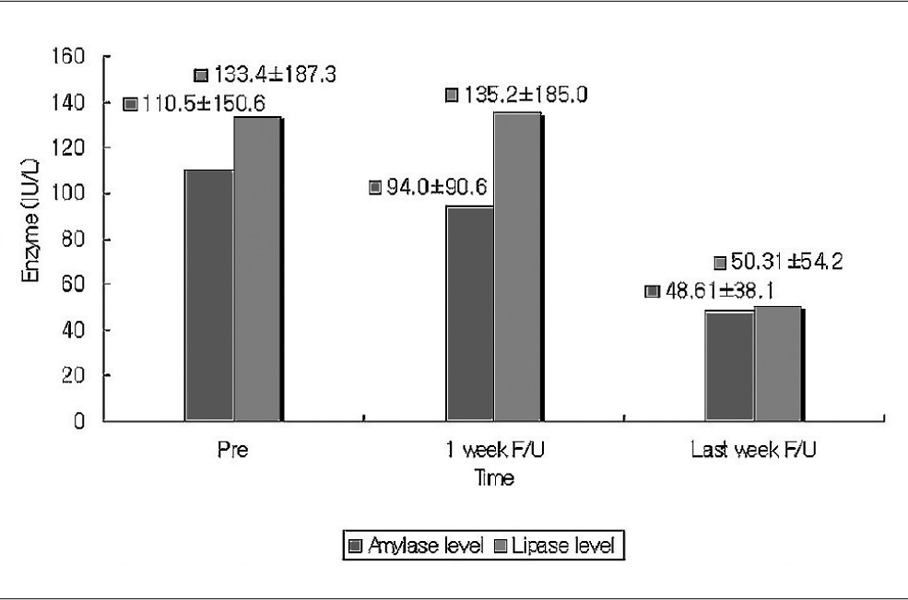
Fig. 3 The graph shows the changes of the amylase and lipase level before and after stent placement and during the last follow-up.
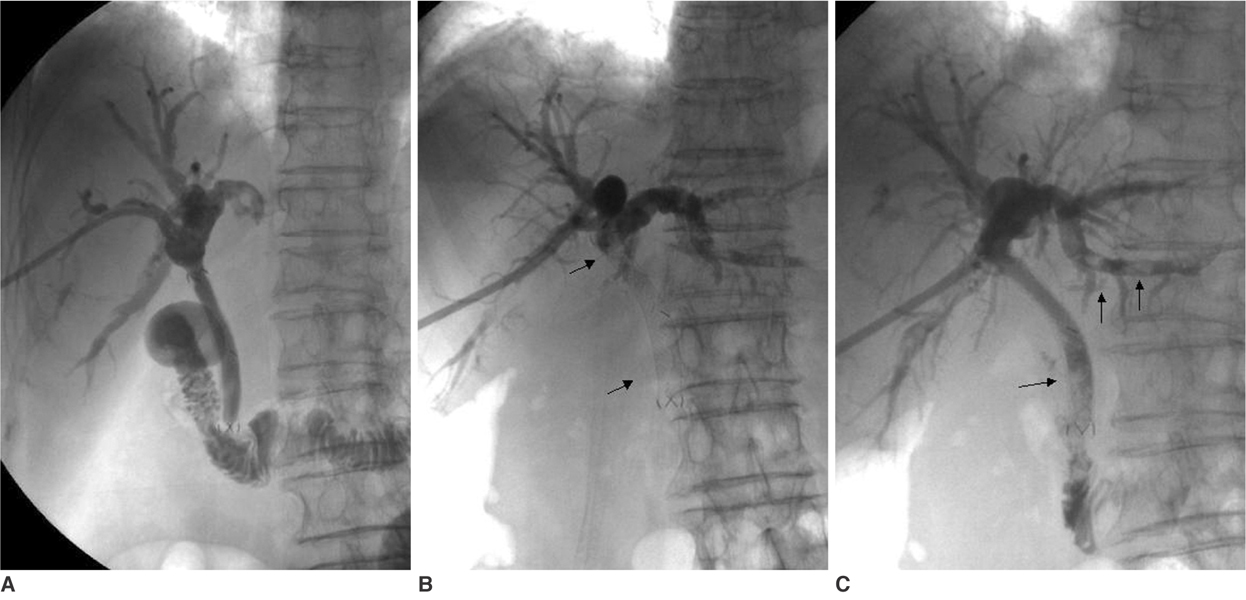
Fig. 4 A 78-year-old female with common bile duct carcinoma. A. The one-week follow-up tubogram shows a well functioning stent. B. This 33-week follow-up tubogram after percutaneous transhepatic biliary drainage shows no contrast medium, due to food reflux, in the stent (arrows). C. The tubogram after stent irrigation shows good passage of contrast medium into the duodenum. Small remnants of food material (arrows) were observed in the left intrahepatic duct and in the distal portion of the stent.
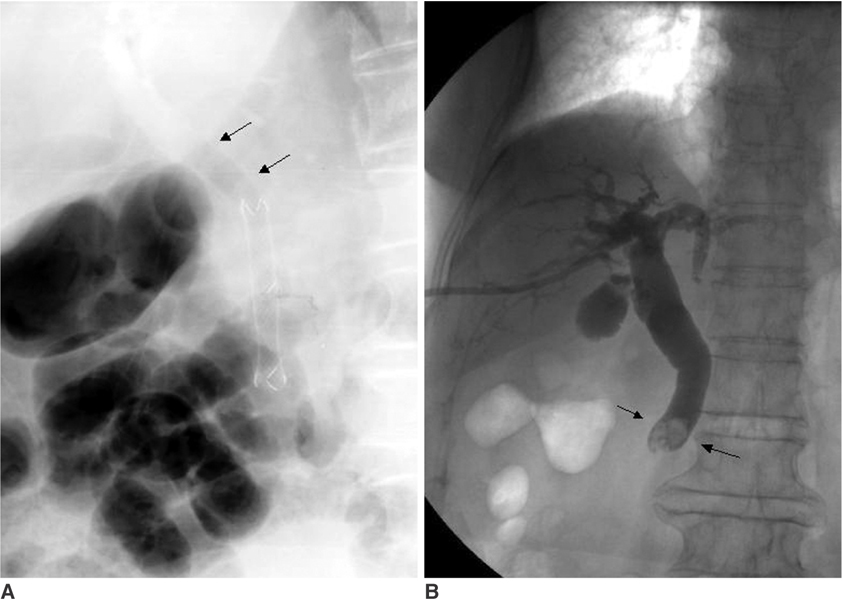
Fig. 5 A 76-year-old female with Ampulla of Vater carcinoma. A. The five-day follow-up plain film after stent insertion shows good stent positioning on the air-biliary gram (arrows). B. The 27-week follow-up tubogram after percutaneous transhepatic biliary drainage shows no evidence for the presence of a stent, and there is a small filling defect in the distal common bile duct, which may be a common bile duct stone (arrows).
Cited by 3 articles
-
Temporary Placement of Stent Grafts in Postsurgical Benign Biliary Strictures: a Single Center Experience
Ranjith Vellody, Jonathon M Willatt, Mohammad Arabi, Wojciech B Cwikiel
Korean J Radiol. 2011;12(6):708-713. doi: 10.3348/kjr.2011.12.6.708.Percutaneous Biliary Drainage Using Open Cell Stents for Malignant Biliary Hilar Obstruction
Sun Jun Ahn, Jae Ik Bae, Tae Sun Han, Je Hwan Won, Ji Dae Kim, Kyu-Sung Kwack, Jae Hee Lee, Young Chul Kim
Korean J Radiol. 2012;13(6):795-802. doi: 10.3348/kjr.2012.13.6.795.Double-Stent System with Long Duodenal Extension for Palliative Treatment of Malignant Extrahepatic Biliary Obstructions: A Prospective Study
Dong Il Gwon, Gi-Young Ko, Jong Woo Kim, Heung Kyu Ko, Hyun-Ki Yoon, Kyu-Bo Sung
Korean J Radiol. 2018;19(2):230-236. doi: 10.3348/kjr.2018.19.2.230.
Reference
-
1. Lammer J, Klein GE, Kleinert R, Hausegger K, Einspieler R. Obstructive jaundice: Use of expandable metal endoprosthesis for biliary drainage. Radiology. 1990. 177:789–792.2. Salomonowitz EK, Adam A, Antonucci F, Stuckmann G, Zollikofer CL. Malignant biliary obstruction: treatment with self expandable stainless steel endoprosthesis. Cardiovas Intervent Radiol. 1992. 15:351–355.3. Gordon RL, Ring EJ, LaBerge JM, Doherty MM. Malignant biliary obstruction: treatment with expandable metallic stents-follow-up of 50 consecutive patients. Radiology. 1992. 182:697–701.4. Laméris JS, Stoker J, Nijs HG, Zonderland HM, Terpstra OT, van Blankenstein M, et al. Malignant biliary obstruction: percutaneous use of self-expandable stents. Radiology. 1991. 179:703–707.5. Rossi P, Bezzi M, Rossi M, Adam A, Chetty N, Roddie ME, et al. Metallic stents in malignant biliary obstruction: results of a multicenter European study of 240 patients. J Vasc Interv Radiol. 1994. 5:279–285.6. Pinol V, Castells A, Bordas JM, Real MI, Llach J, Montana X, et al. Percutaneous self-expanding metal stents versus endoscopic polyethylene endoprostheses for treating malignant biliary obstruction: randomized clinical trial. Radiology. 2002. 225:27–34.7. Boguth L, Tatalovic S, Antonucci F, Heer M, Sulser H, Zollikofer CL. Malignant biliary obstruction: clinical and histopathologic correlation after treatment with self-expanding metal prostheses. Radiology. 1994. 192:669–674.8. Hausegger KA, Kleinert R, Lammer J, Klein GE, Fluckiger F. Malignant biliary obstruction: histologic findings after treatment with self-expandable stents. Radiology. 1992. 185:461–464.9. Eschelman DJ, Shapiro MJ, Bonn J, Sullivan KL, Alden ME, Hovsepian DM, et al. Malignant biliary duct obstruction: long-term experience with Gianturco stents and combined-modality radiation therapy. Radiology. 1996. 200:717–724.10. Hausegger KA, Thurnher S, Bodendörfer G, Zollikofer CL, Uggowitzer M, Kugler C, et al. Treatment of malignant biliary obstruction with polyurethane-covered Wallstents. AJR Am J Roentgeonl. 1998. 170:403–408.11. Nakamura T, Kitagawa M, Takehira Y, Yamada M, Kawasaki T, Nakamura H. Polyurethane-covered Wallstents to recanalize Wallstents obstructed by tumor ingrowth from malignant common bile duct obstruction. Cardiovasc Intervent Radiol. 2000. 23:161–164.12. Kanasaki S, Furukawa A, Kane T, Murata K. Polyurethane-covered Nitinol Strecker stents as primary palliative treatment of malignant biliary obstruction. Cardiovasc Intervent Radiol. 2000. 23:114–120.13. Han YM, Hwang SB, Lee ST, Lee JM, Chung GH. Polyurethane-covered self-expandable nitinol stent for malignant biliary obstruction: preliminary results. Cardiovasc Intervent Radiol. 2002. 25:381–387.14. Born P, Neuhaus H, Rösch T, Ott R, Allescher H, Frimberger E, et al. Initial experience with a new, partially covered Wallstent for malignant biliary obstruction. Endoscopy. 1996. 28:699–702.15. Thurnher SA, Lammer J, Thurnher MM, Winkelbauer F, Graf O, Wildling R. Covered self-expanding transhepatic biliary stents: clinical pilot study. Cardiovasc Intervent Radiol. 1996. 19:10–14.16. Rossi P, Bezzi M, Salvatori FM, Panzetti C, Rossi M, Pavia G. Clinical experience with covered Wallstents for biliary malignancies: 23-month follow-up. Cardiovasc Intervent Radiol. 1997. 20:441–447.17. Miyayama S, Matsui O, Terayama N, Tatsu H, Yamamoto T, Takashima T. Covered Gianturco stents for malignant biliary obstruction: preliminary clinical evaluation. J Vasc Interv Radiol. 1997. 8:641–648.18. Bezzi M, Zolovkins A, Cantisani V, Salvatori FM, Rossi M, Fanelli F, et al. New ePTFE/FEP-covered stent in the palliative treatment of malignant biliary obstruction. J Vasc Interv Radiol. 2002. 13:581–589.19. Schoder M, Rossi P, Uflacker R, Bezzi M, Stadler A, Funovics MA, et al. Malignant biliary obstruction: treatment with ePTFE-FEP-covered endoprostheses initial technical and clinical experiences in a multicenter trial. Radiology. 2002. 225:35–42.20. Han YM, Jin GY, Lee SO, Kwak HS, Chung GH. Flared polyurethane-covered self-expandable nitinol stent for malignant biliary obstruction. J Vasc Interv Radiol. 2003. 14:1291–1301.21. Zografakis JG, Jones BT, Ravichardran P, Evancho-Chapman MM, Schmidt SP, Arends D, et al. Endoluminal reconstruction of the canine common biliary duct. Curr Surg. 2003. 60:437–441.22. Lammer J, Stöffler G, Petek WW, Höfler H. In vitro long-term perfusion of different materials for biliary endoprostheses. Invest Radiol. 1986. 21:329–331.23. Vanderburgh L, Ho CS. Nonvascualar stents. Pro Cardiovasc Dis. 1996. 39:187–200.24. Isayama H, Komatsu Y, Tsujino T, Sasahira N, Hirano K, Toda N, et al. A prospective randomized study of "covered" versus "uncovered" diamond stents for management of distal malignant biliary obstruction. Gut. 2004. 53:729–734.25. Yoon WJ, Lee JK, Lee KH, Lee WJ, Ryu JK, Kim YT, et al. A comparison of covered and uncovered Wallstents for the management of distal malignant biliary obstruction. Gastrointest Endosc. 2006. 63:996–1000.26. Park DH, Kim MH, Choi JS, Lee SS, Seo DW, Kim JH, et al. Covered versus uncovered Wallstent for malignant extrahepatic biliary obstruction: a cohort comparative analysis. Clin Gastroenterol Hepatol. 2006. 4:790–796.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Self-Expandable Polytetrafluoroethylene (PTFE)-covered Nitinol Stent for the Palliative Treatment of Malignant Biliary Obstruction
- Malignant Duodenal Obstructions: Palliative Treatment with Covered Expandable Nitinol Stent
- A Dual Expandable Nitinol Stent: The Long-term Results in Patients with Malignant Gastroduodenal Strictures
- Treatment of Malignant Gastroduodenal Obstruction with Using a Newly Designed Complex Expandable Nitinol Stent: Initial Experiences
- Proximal Stent Migration of Fully Covered Self-Expandable Metal Stent following Side-by-Side Deployment in the Patient with Klatskin Tumor: A Case Report
