(18)F-FDG PET versus (18)F-FDG PET/CT for Adrenal Gland Lesion Characterization: a Comparison of Diagnostic Efficacy in Lung Cancer Patients
- Affiliations
-
- 1Department of Radiology and Center for Imaging Science, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. kyungs.lee@samsung.com
- 2Department of Medical Imaging, Toronto General Hospital, University Health Network, Toronto, Ontario, Canada.
- 3Department of Nuclear Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 4Department of Thoracic Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 1734271
- DOI: http://doi.org/10.3348/kjr.2008.9.1.19
Abstract
OBJECTIVE
The aim of this study was to assess the diagnostic efficacy of integrated PET/CT using fluorodeoxyglucose (FDG) for the differentiation of benign and metastatic adrenal gland lesions in patients with lung cancer and to compare the diagnostic efficacy with the use of PET alone. MATERIALS AND METHODS: Sixty-one adrenal lesions (size range, 5-104 mm; mean size, 16 mm) were evaluated retrospectively in 42 lung cancer patients. Both PET images alone and integrated PET/CT images were assessed, respectively, at two-month intervals. PET findings were interpreted as positive if the FDG uptake of adrenal lesions was greater than or equal to that of the liver, and the PET/CT findings were interpreted as positive if an adrenal lesion show attenuation > 10 HU and showed increased FDG uptake. Final diagnoses of adrenal gland lesions were made at clinical follow-up (n = 52) or by a biopsy (n = 9) when available. The diagnostic accuracies of PET and PET/CT for the characterization of adrenal lesions were compared using the McNemar test. RESULTS: Thirty-five (57%) of the 61 adrenal lesions were metastatic and the remaining 26 lesions were benign. For the depiction of adrenal gland metastasis, the sensitivity, specificity, and accuracy of PET were 74%, 73%, and 74%, respectively, whereas those of integrated PET/CT were 80%, 89%, and 84%, respectively (p values; 0.5, 0.125, and 0.031, respectively). CONCLUSION: The use of integrated PET/CT is more accurate than the use of PET alone for differentiating benign and metastatic adrenal gland lesions in lung cancer patients.
Keyword
MeSH Terms
-
Adrenal Gland Neoplasms/pathology/*radiography/*radionuclide imaging/secondary
Adult
Aged
Biopsy
Diagnosis, Differential
Female
Fluorodeoxyglucose F18/*diagnostic use
Humans
Lung Neoplasms/pathology/*radiography/*radionuclide imaging
Male
Middle Aged
Positron-Emission Tomography/*methods
Radiopharmaceuticals/*diagnostic use
Retrospective Studies
Sensitivity and Specificity
Tomography, X-Ray Computed/*methods
Figure
-
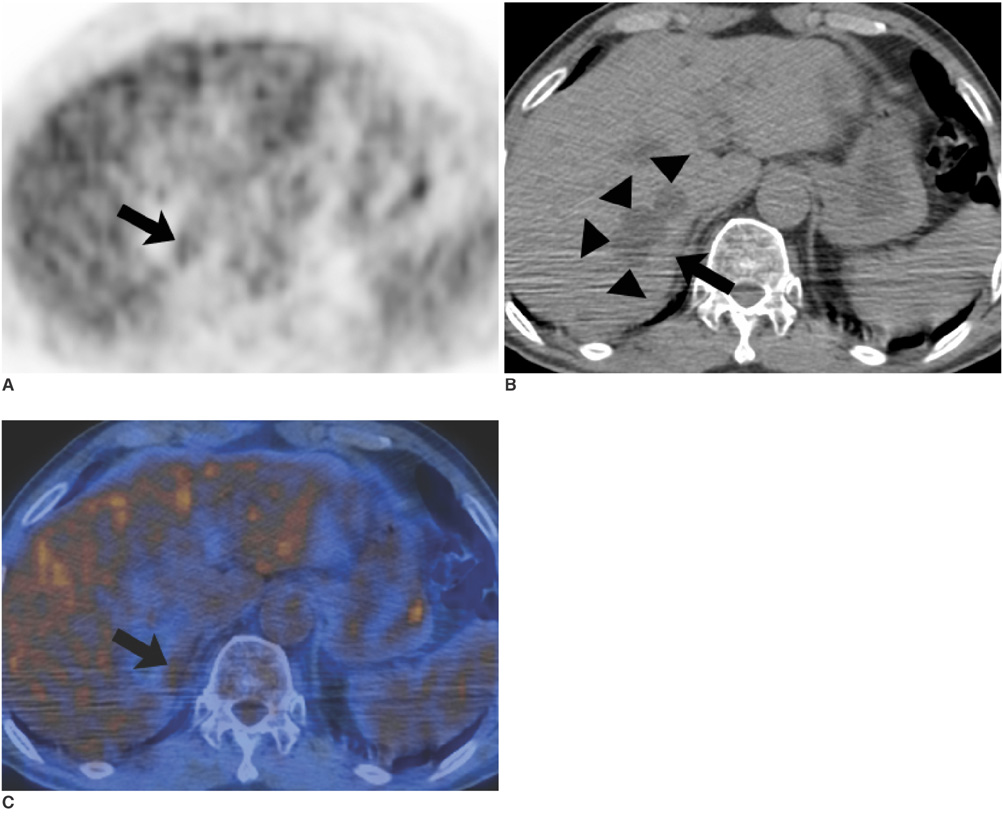
Fig. 1 A false-positive interpretation with the use of PET only, but a true negative interpretation with the use of integrated PET/CT in a 57-year-old man with adenocarcinoma in the right upper lobe of the lung. A. PET demonstrates increased uptake (arrow) in the right adrenal gland area with a maximum standardized uptake value of 3.2. PET alone regarded the uptake as positive. B. Unenhanced CT scan shows hepatic cysts (arrowheads). C. On an integrated PET/CT image, the uptake (arrow) falls on the liver, thus enabling a correct interpretation as negative uptake in the right adrenal gland.
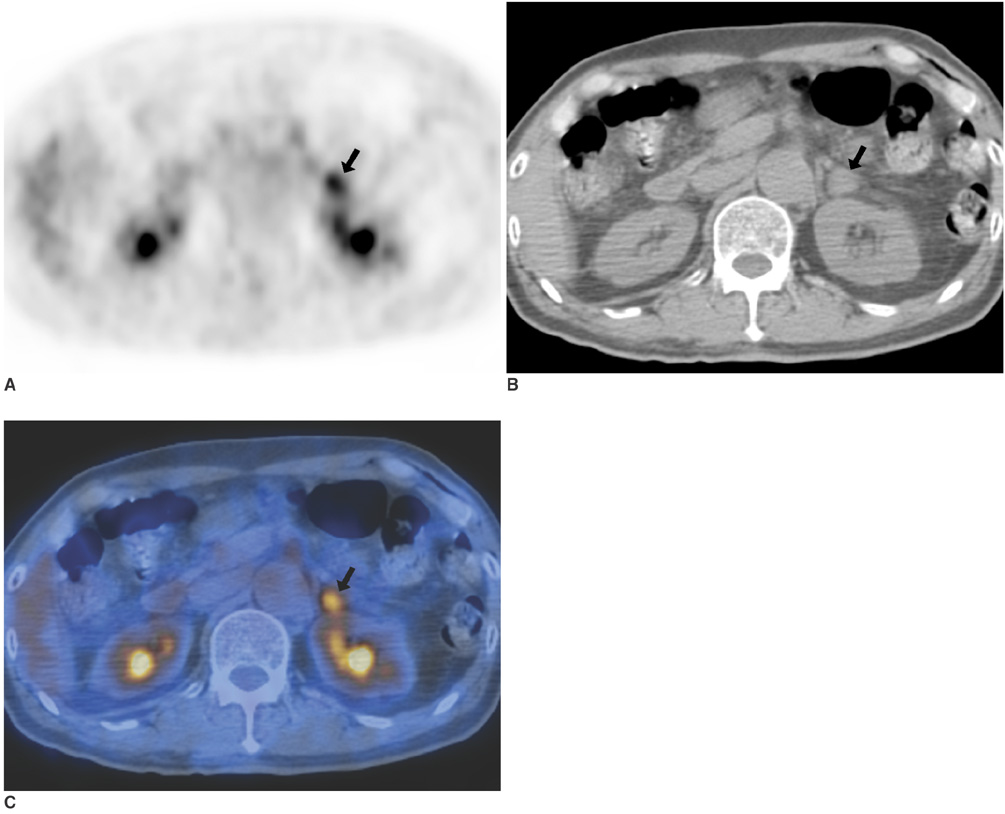
Fig. 2 A false-positive interpretation by the use of both PET and PET/CT in a 33-year-old woman with an adrenal adenoma that was confirmed by surgical excision. The patient also had an adenocarcinoma in the left lower lobe of the lung. A. PET demonstrates increased uptake (arrow) in the left adrenal gland lesion with a maximum standardized uptake value of 4.6. B. An unenhanced CT scan shows a 14 mm sized nodule (arrow) in the left adrenal gland. C. Integrated PET/CT shows high uptake (arrow) in the nodule of the left adrenal gland.
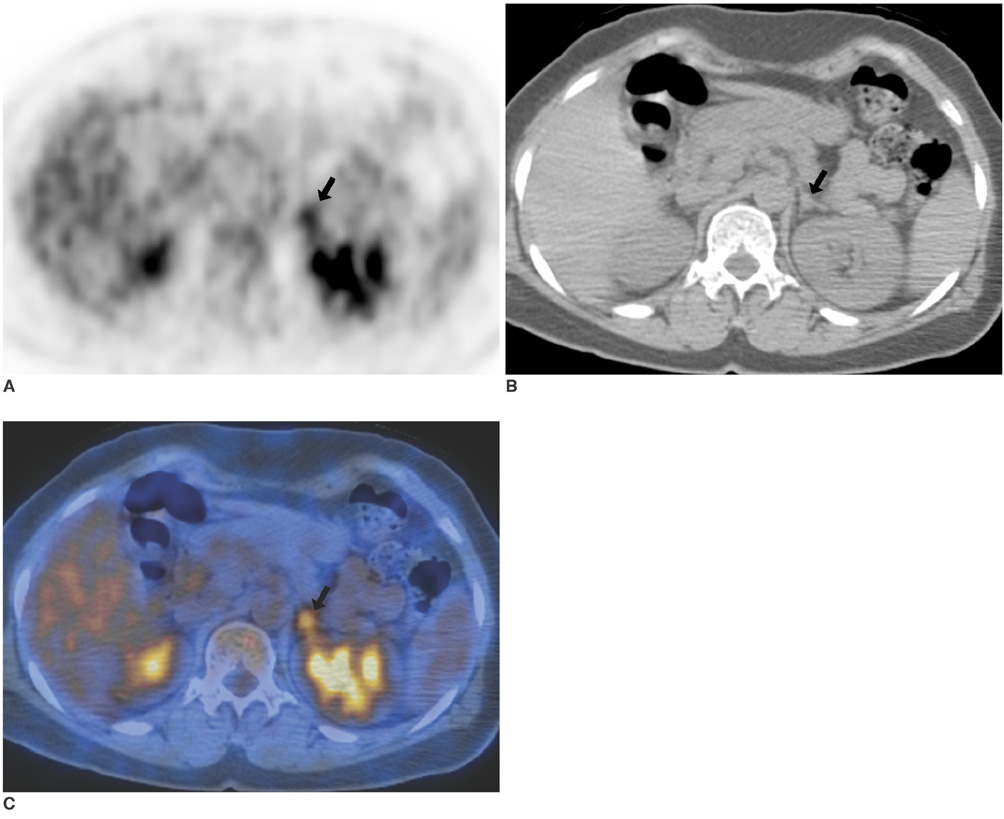
Fig. 3 A false-positive interpretation by the use of both PET and PET/CT in a 56-year-old woman with an endothelial cyst that was confirmed by surgical excision. The patient also had a squamous cell carcinoma in the left lower lobe of the lung. A. PET demonstrates increased uptake (arrow) in the left adrenal gland lesion with a maximum standardized uptake value of 4.3. B. An unenhanced CT scan shows a 7 mm sized nodule (arrow) in the left adrenal gland. C. Integrated FDG PET/CT shows high uptake (arrow) in the nodule of the left adrenal gland.
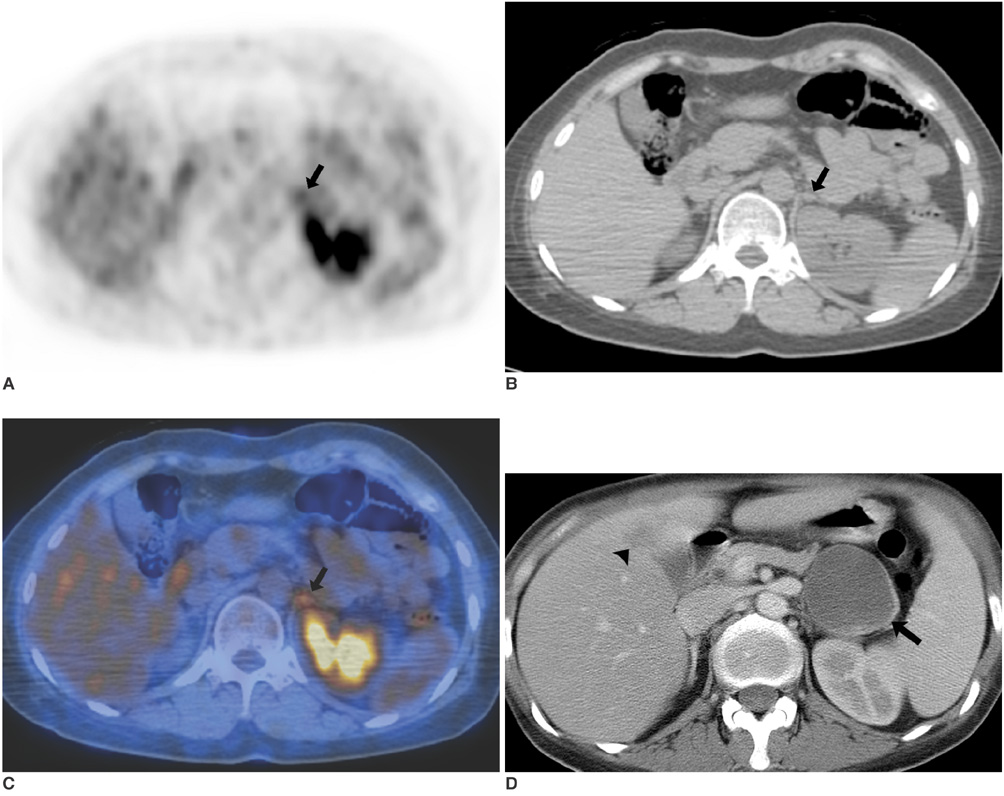
Fig. 4 A false-negative interpretation with the use of PET only, but a true positive interpretation with the use of integrated PET/CT in a 33-year-old woman with an adrenal metastasis confirmed by clinical follow-up. The patient also had adenocarcinoma in the right lower lobe of the lung. A. PET demonstrates increased uptake (arrow) in the left adrenal gland area with a maximum SUV of 3.5. Uptake was regarded as benign by PET alone because the uptake was interpreted as left kidney uptake. B. An unenhanced CT scan shows an 11-mm-sized nodule (arrow) in the left adrenal gland. C. On an integrated PET/CT image, the uptake (arrow) falls on the left adrenal gland, thus enabling a correct interpretation as positive uptake (uptake extent is equal to that of liver). D. The nodule (arrow) in the left adrenal gland shows an increase in size at a 7-month follow-up CT. Hepatic metastasis is also noted (arrowhead).
Reference
-
1. Ettinghausen SE, Burt ME. Prospective evaluation of unilateral adrenal masses in patients with operable non-small-cell lung cancer. J Clin Oncol. 1991. 9:1462–1466.2. Hedeland H, Ostberg G, Hokfelt B. On the prevalence of adrenocortical adenomas in an autopsy material in relation to hypertension and diabetes. Acta Med Scand. 1968. 184:211–214.3. Chapman GS, Kumar D, Redmond J 3rd, Munderloh SH, Gandara DR. Upper abdominal computerized tomography scanning in staging non-small cell lung carcinoma. Cancer. 1984. 54:1541–1543.4. Abrams HL, Spiro R, Goldstein N. Metastases in carcinoma; analysis of 1000 autopsied cases. Cancer. 1950. 3:74–85.5. Oliver TW Jr, Bernardino ME, Miller JI, Mansour K, Greene D, Davis WA. Isolated adrenal masses in nonsmall-cell bronchogenic carcinoma. Radiology. 1984. 153:217–218.6. Herrera MF, Grant CS, van Heerden JA, Sheedy PF, Ilstrup DM. Incidentally discovered adrenal thmors: an institutional perspective. Surgery. 1991. 110:1014–1021.7. Porte HL, Roumilhac D, Graziana JP, Eraldi L, Cordonier C, Puech P, et al. Adrenalectomy for a solitary adrenal metastasis from lung cancer. Ann Thorac Surg. 1998. 65:331–335.8. Burt M, Heelan RT, Coit D, McCormack PM, Bains MS, Martini N, et al. Prospective evaluation of unilateral adrenal masses in patients with operable non-small-cell lung cancer. Impact of magnetic resonance imaging. J Thorac Cardiovasc Surg. 1994. 107:584–589.9. Mody MK, Kazerooni EA, Korobkin M. Percutaneous CT-guided biopsy of adrenal masses: immediate and delayed complications. J Comput Assist Tomogr. 1995. 19:434–439.10. Namimoto T, Yamashita Y, Mitsuzuki K, Nakayama Y, Makita O, Kadota M, et al. Adrenal masses: quantification of fat content with double-echo chemical shift in-phase and opposed-phase FLASH MR images for differentiation of adrenal adenomas. Radiology. 2001. 218:642–646.11. Tsushima Y, Ishizaka H, Matsumoto M. Adrenal masses: differentiation with chemical shift, fast low-angle shot MR imaging. Radiology. 1993. 186:705–709.12. Caoili EM, Korobkin M, Francis IR, Cohan RH, Platt JF, Dunnick NR, et al. Adrenal masses: characterization with combined unenhanced and delayed enhanced CT. Radiology. 2002. 222:629–633.13. Lee MJ, Hahn PF, Papanicolaou N, Egglin TK, Saini S, Mueller PR, et al. Benign and malignant adrenal masses: CT distinction with attenuation coefficients, size, and observer analysis. Radiology. 1991. 179:415–418.14. Pena CS, Boland GW, Hahn PF, Lee MJ, Mueller PR. Characterization of indeterminate (lipid-poor) adrenal masses: use of washout characteristics at contrast-enhanced CT. Radiology. 2000. 217:798–802.15. Kumar R, Xiu Y, Yu JQ, Takalkar A, El-Haddad G, Potenta S, et al. 18F-FDG PET in evaluation of adrenal lesions in patients with lung cancer. J Nucl Med. 2004. 45:2058–2062.16. Erasmus JJ, Patz EF Jr, McAdams HP, Murray JG, Herndon J, Coleman RE, et al. Evaluation of adrenal masses in patients with bronchogenic carcinoma using 18F-fluorodeoxyglucose positron emission tomography. AJR Am J Roentgenol. 1997. 168:1357–1360.17. Boland GW, Goldberg MA, Lee MJ, Mayo-Smith WW, Dixon J, McNicholas MM, et al. Indeterminate adrenal mass in patients with cancer: evaluation at PET with 2-[F-18]-fluoro-2-deoxy-D-glucose. Radiology. 1995. 194:131–134.18. Yun M, Kim W, Alnafisi N, Lacorte L, Jang S, Alavi A. 18F-FDG PET in characterizing adrenal lesions detected on CT or MRI. J Nucl Med. 2001. 42:1795–1799.19. Gupta NC, Graeber GM, Tamim WJ, Rogers JS, Irisari L, Bishop HA. Clinical utility of PET-FDG imaging in differentiation of benign from malignant adrenal masses in lung cancer. Clin Lung Cancer. 2001. 3:59–64.20. Maurea S, Mainolfi C, Bazzicalupo L, Panico MR, Imparato C, Alfano B, et al. Imaging of adrenal tumors using FDG PET: comparison of benign and malignant lesions. AJR Am J Roentgenol. 1999. 173:25–29.21. Beyer T, Townsend DW, Brun T, Kinahan PE, Charron M, Roddy R, et al. A combined PET/CT scanner for clinical oncology. J Nucl Med. 2000. 41:1369–1379.22. Townsend DW, Beyer T, Blodgett TM. PET/CT scanners: a hardware approach to image fusion. Semin Nucl Med. 2003. 33:193–204.23. Townsend DW. A combined PET/CT scanner: the choices. J Nucl Med. 2001. 42:533–534.24. von Schulthess GK. Positron emission tomography versus positron emission tomography/computed tomography: from "unclear" to "new-clear" medicine. Mol Imaging Biol. 2004. 6:183–187.25. Messa C, Bettinardi V, Picchio M, Pelosi E, Landoni C, Gianolli L, et al. PET/CT in diagnostic oncology. Q J Nucl Med Mol Imaging. 2004. 48:66–75.26. Pelosi E, Messa C, Sironi S, Picchio M, Landoni C, Bettinardi V, et al. Value of integrated PET/CT for lesion localisation in cancer patients: a comparative study. Eur J Nucl Med Mol Imaging. 2004. 31:932–939.27. Cerfolio RJ, Ojha B, Bryant AS, Raghuveer V, Mountz JM, Bartolucci AA. The accuracy of integrated PET-CT compared with dedicated PET alone for the staging of patients with nonsmall cell lung cancer. Ann Thorac Surg. 2004. 78:1017–1023.28. Costa DC, Visvikis D, Crosdale I, Pigden I, Townsend C, Bomanji J, et al. Positron emission and computed X-ray tomography: a coming together. Nucl Med Commun. 2003. 24:351–358.29. Lardinois D, Weder W, Hany TF, Kamel EM, Korom S, Seifert B, et al. Staging of non-small-cell lung cancer with integrated positron-emission tomography and computed tomography. N Engl J Med. 2003. 348:2500–2507.30. Bar-Shalom R, Yefremov N, Guralnik L, Gaitini D, Frenkel A, Kuten A, et al. Clinical performance of PET/CT in evaluation of cancer: additional value for diagnostic imaging and patient management. J Nucl Med. 2003. 44:1200–1209.31. Hany TF, Steinert HC, Goerres GW, Buck A, von Schulthess GK. PET diagnostic accuracy: improvement with in-line PET-CT system: initial results. Radiology. 2002. 225:575–581.32. Metser U, Miller E, Lerman H, Lievshitz G, Avital S, Even-Sapir E. 18F-FDG PET/CT in the evaluation of adrenal masses. J Nucl Med. 2006. 47:32–37.33. Blake MA, Slattery JM, Kalra MK, Halpern EF, Fischman AJ, Mueller PR, et al. Adrenal lesions: characterization with fused PET/CT image in patients with proved or suspected malignancy-initial experience. Radiology. 2006. 238:970–997.34. Haider MA, Ghai S, Jhaveri K, Lockwood G. Chemical shift MR imaging of hyperattenuating (>10 HU) adrenal masses: does it still have a role? Radiology. 2004. 231:711–771.35. Bagheri B, Maurer AH, Cone L, Doss M, Adler L. Characterization of the normal adrenal gland with 18F-FDG PET/CT. J Nucl Med. 2004. 45:1340–1343.36. Shulkin BL, Thompson NW, Shapiro B, Francis IR, Sisson JC. Pheochromocytomas: imaging with 2-[fluorine-18] fluoro-2-deoxy-D-glucose PET. Radiology. 1999. 212:35–41.37. Erasmus JJ, McAdams HP, Patz EF Jr, Coleman RE, Ahuja V, Goodman PC. Evaluation of primary pulmonary carcinoid tumors using FDG PET. AJR Am J Roentgenol. 1998. 170:1369–1373.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Incidentally Detected Nasopharyngeal Tuberculosis on F-18 FDG PET/CT
- High FDG Uptake in Sclerosing Hemangioma
- Differential Diagnosis of Breast Mass and Staging of Breast Cancer Using F-18-FDG PET
- F-18 FDG PET/CT Finding in Solid Pseudo-papillary Tumor of the Pancreas 6 years After Initial Diagnosis
- Retroperitoneal Pleomorphic Liposarcoma Mimicking Adrenal Cancer in F-18 FDG PET/CT
