Anatomy, Variants, and Pathologies of the Superior Glenohumeral Ligament: Magnetic Resonance Imaging with Three-Dimensional Volumetric Interpolated Breath-Hold Examination Sequence and Conventional Magnetic Resonance Arthrography
- Affiliations
-
- 1Department of Radiology, Medical Faculty, Ataturk University, Erzurum 25090, Turkey. drhogul@gmail.com
- 2Department of Orthopedic, Medical Faculty, Ataturk University, Erzurum 25090, Turkey.
- KMID: 1731056
- DOI: http://doi.org/10.3348/kjr.2014.15.4.508
Abstract
- The purpose of this review was to demonstrate magnetic resonance (MR) arthrography findings of anatomy, variants, and pathologic conditions of the superior glenohumeral ligament (SGHL). This review also demonstrates the applicability of a new MR arthrography sequence in the anterosuperior portion of the glenohumeral joint. The SGHL is a very important anatomical structure in the rotator interval that is responsible for stabilizing the long head of the biceps tendon. Therefore, a torn SGHL can result in pain and instability. Observation of the SGHL is difficult when using conventional MR imaging, because the ligament may be poorly visualized. Shoulder MR arthrography is the most accurately established imaging technique for identifying pathologies of the SGHL and associated structures. The use of three dimensional (3D) volumetric interpolated breath-hold examination (VIBE) sequences produces thinner image slices and enables a higher in-plane resolution than conventional MR arthrography sequences. Therefore, shoulder MR arthrography using 3D VIBE sequences may contribute to evaluating of the smaller intraarticular structures such as the SGHL.
Keyword
MeSH Terms
Figure
-
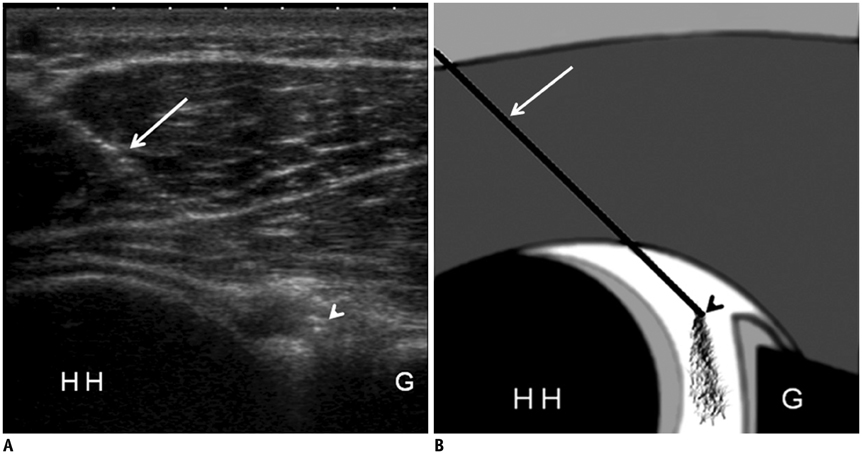
Fig. 1 Ultrasonography-guided posterior injection technique for shoulder MR arthrography. A. Transverse ultrasonography image shows needle track and intraarticular needle tip in patient with posterior glenohumeral joint puncture for MR arthrography. It also reveals distention of joint capsule with free fluid within joint space. White arrow = needle shaft, white arrowhead = intraarticular needle tip. B. Corresponding schematic drawing shows optimal needle track and placement. White arrow = needle shaft, black arrowhead = intraarticular needle tip. G = posterior glenoid rim, HH = humeral head
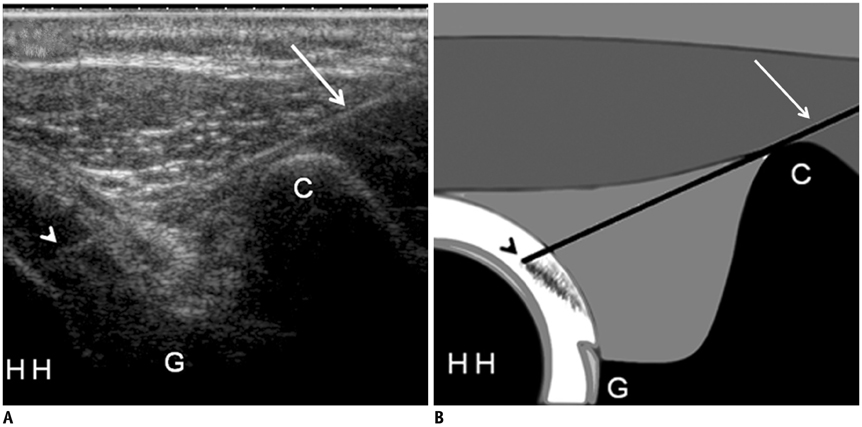
Fig. 2 Ultrasonography-guided rotator interval injection technique for shoulder MR arthrography. A. Axial oblique ultrasonography image, obtained at anterosuperior aspect of glenohumeral joint, shows needle track (white arrow) and intraarticular needle tip (white arrowhead) in patient with rotator interval puncture for MR arthrography. Image also shows distention of joint capsule with free fluid within joint space. B. Corresponding schematic drawing shows optimal needle track and placement. White arrow = needle shaft, black arrowhead = intraarticular needle tip. C = coracoid process, G = anterior glenoid rim, HH = humeral head

Fig. 3 Normal arthrographic anatomy of SGHL in 51-year-old male who suffered from shoulder pain. A. Axial reformatted image of fat-suppressed 3D VIBE sequence shows SGHL (black arrow). B. Oblique sagittal reformatted image of fat-suppressed 3D VIBE sequence shows SGHL (black arrow) underneath coracoid process. C. Oblique sagittal fat-saturated 3D VIBE MR arthrographic image shows normal anatomic appearance of pulley sling. SGHL (white arrow) wraps around horizontal portion of LHBT (black dotted arrow), which is at distance from subscapularis tendon (SSC). LHBT shows normal diameter and signal intensity. LHBT = long head of biceps tendon, SGHL = superior glenohumeral ligament, 3D VIBE = three-dimensional volumetric interpolated breath-hold examination
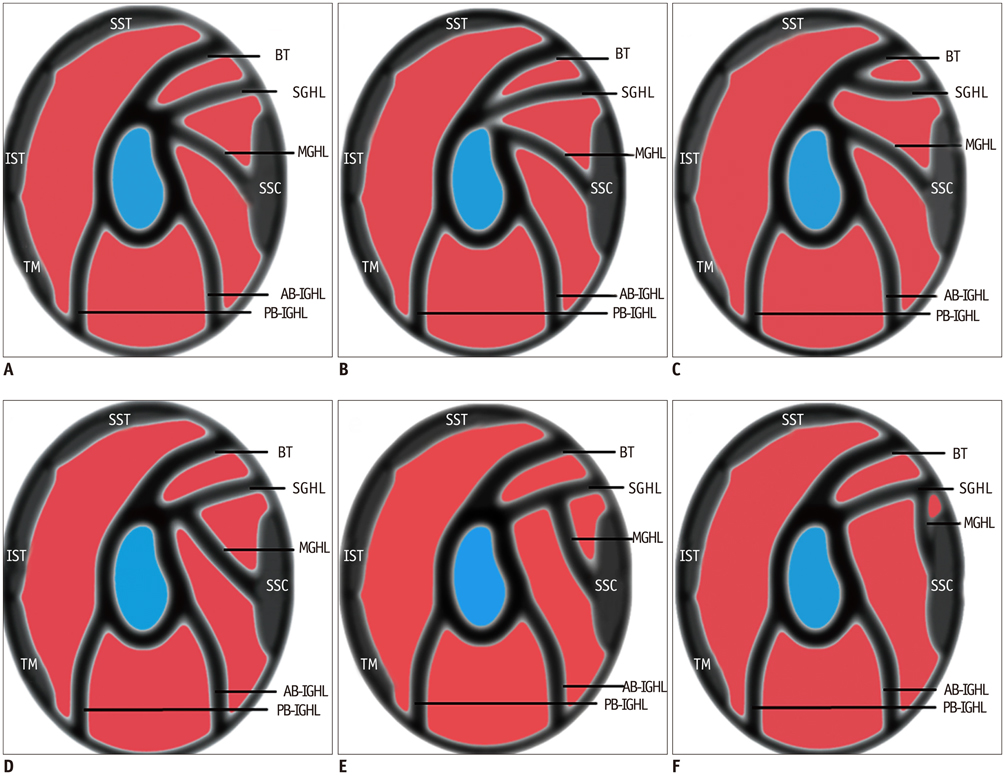
Fig. 4 Types of SGHL origination. A. Drawing (lateral view) shows normal anatomy of glenohumeral ligaments. Figure also shows origination of SGHL from anterior supraglenoid tubercle. B. Drawing shows origination of SGHL from posterior supraglenoid tubercle. C. Drawing shows SGHL originating with LHBT. D-F. Drawings show types of conjugation of SGHL with MGHL. AB-IGHL = anterior band of inferior glenohumeral ligament, BT = long head of biceps tendon, IST = infraspinatus tendon, MGHL = middle glenohumeral ligament, PB-IGHL = posterior band of inferior glenohumeral ligament, SGHL = superior glenohumeral ligament, SSC = subscapularis tendon, SST = supraspinatus tendon, TM = teres minor tendon
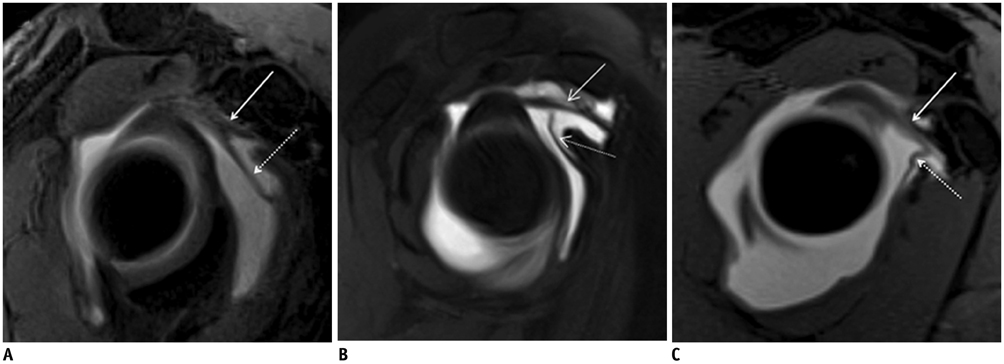
Fig. 5 Types of conjugation of SGHL with MGHL in three different patients. A. Oblique sagittal fat-saturated 3D VIBE MR arthrographic image shows distal conjugation of SGHL (white arrow) with MGHL (white dotted arrow). B. Oblique sagittal fat-saturated 3D VIBE MR arthrographic image shows conjugation in mid segment of SGHL (white arrow) with MGHL (white dotted arrow). C. Oblique sagittal fat-saturated 3D VIBE MR arthrographic image shows proximal conjugation of SGHL (white arrow) with MGHL (white dotted arrow). MGHL = middle glenohumeral ligament, SGHL = superior glenohumeral ligament, 3D VIBE = three-dimensional volumetric interpolated breath-hold examination

Fig. 6 Origination from posterior supraglenoid tubercle of SGHL with LHBT, in 32-year-old woman who suffered from shoulder pain. Consecutive axial fat-saturated T1-weighted MR arthrographic images show origination of SGHL (black arrow) with LHBT (white dotted arrow) from posterior supraglenoid tubercle. Linear focus of contrast material extending into sublabral sulcus (white arrowhead) is noted. LHBT = long head of biceps tendon, SGHL = superior glenohumeral ligament

Fig. 7 Origination of SGHL from both anterior supraglenoid tubercle and LHBT, in 29-year-old woman who suffered from shoulder pain. A, B. Consecutive axial fat-saturated T1-weighted MR arthrographic images show origination (white arrowhead) of SGHL (white arrow) from both anterior supraglenoid tubercle and LHBT (white dotted arrow). C. Oblique sagittal T1-weighted MR arthrographic image shows fan-shaped insertion (white arrowhead) of SGHL (white arrow) into LHBT (white dotted arrow). LHBT = long head of biceps tendon, SGHL = superior glenohumeral ligament

Fig. 8 Types of variations in shape and size of SGHL. A. Drawing (lateral view) shows thick SGHL and absent MGHL. B. Drawing shows thick SGHL and thin MGHL. C. Drawing shows double SGHL. D. Drawing shows absent SGHL. AB-IGHL = anterior band of inferior glenohumeral ligament, BT = long head of biceps tendon, IST = infraspinatus tendon, MGHL = middle glenohumeral ligament, PB-IGHL = posterior band of inferior glenohumeral ligament, SGHL = superior glenohumeral ligament, SSC = subscapularis tendon, SST = supraspinatus tendon, TM = teres minor tendon

Fig. 9 Thick SGHL and absence of MGHL in 47-year-old woman who suffered from chronic shoulder pain. Oblique sagittal and axial fat-saturated 3D VIBE MR arthrographic images showing thick SGHL (white arrow) and absence of MGHL. MGHL = middle glenohumeral ligament, SGHL = superior glenohumeral ligament, 3D VIBE = three-dimensional volumetric interpolated breath-hold examination
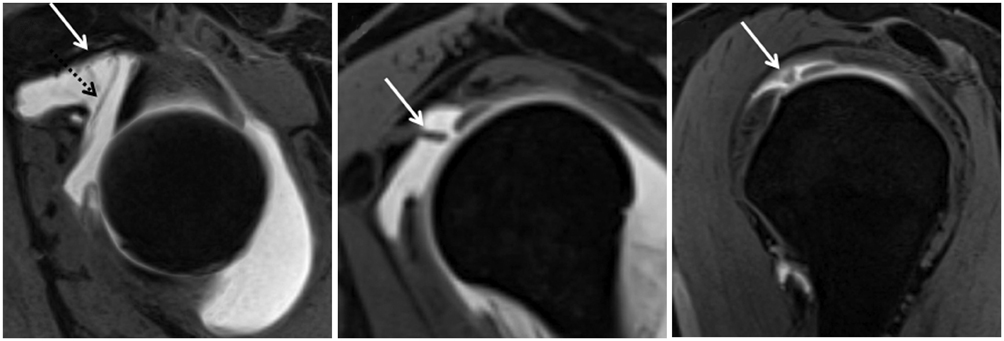
Fig. 10 Thick SGHL and thin MGHL in 43-year-old man who suffered from shoulder pain. Consecutive oblique sagittal fat-saturated 3D VIBE MR arthrographic images show thick SGHL (white arrow) and thin MGHL (black dotted arrow). MGHL = middle glenohumeral ligament, SGHL = superior glenohumeral ligament, 3D VIBE = three-dimensional volumetric interpolated breath-hold examination
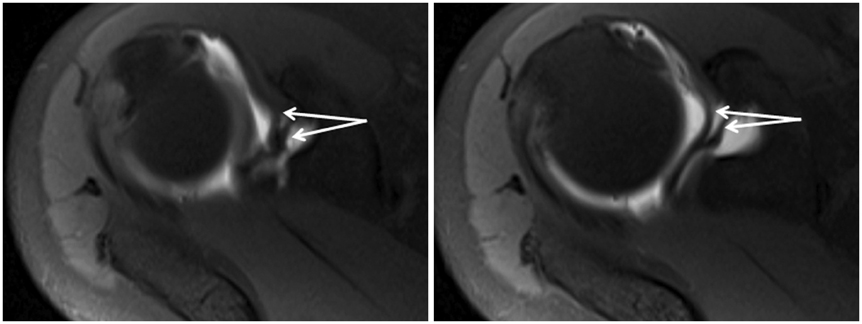
Fig. 11 Double SGHL in 31-year-old woman who suffered from shoulder pain. Consecutive axial fat-saturated T1-weighted MR arthrographic images show double SGHL (white arrows). SGHL = superior glenohumeral ligament
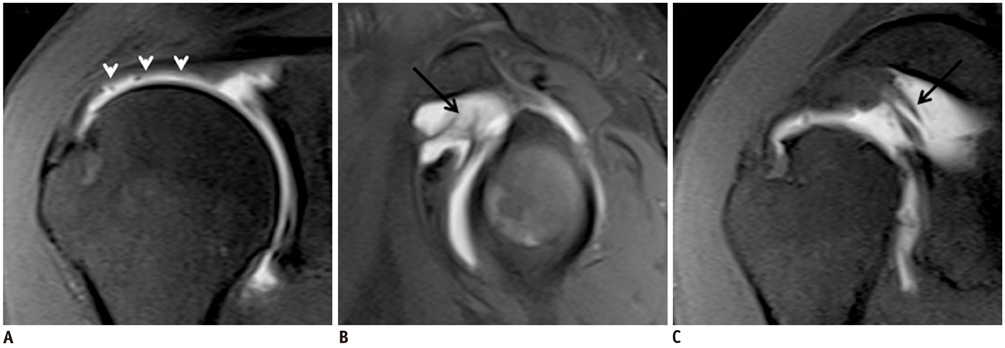
Fig. 12 Partial tear of undersurface of supraspinatus tendon with SGHL tear in 47-year-old man. A. Oblique coronal fat-saturated T1-weighted MR arthrographic image shows partial tear of undersurface of supraspinatus tendon (white arrowheads). B, C. Oblique sagittal and oblique coronal fat-saturated T1-weighted MR arthrographic images show SGHL tear (black arrow). SGHL = superior glenohumeral ligament

Fig. 13 Habermeyer group 1 lesion in 45-year-old man. Axial fat-saturated T1-weighted and oblique sagittal fat-saturated 3D VIBE MR arthrographic images show isolated superior GHL tear (white arrow). White dotted arrow = LHBT. GHL = glenohumeral ligament, LHBT = long head of biceps tendon, SSC = subscapularis tendon, 3D VIBE = three-dimensional volumetric interpolated breath-hold examination
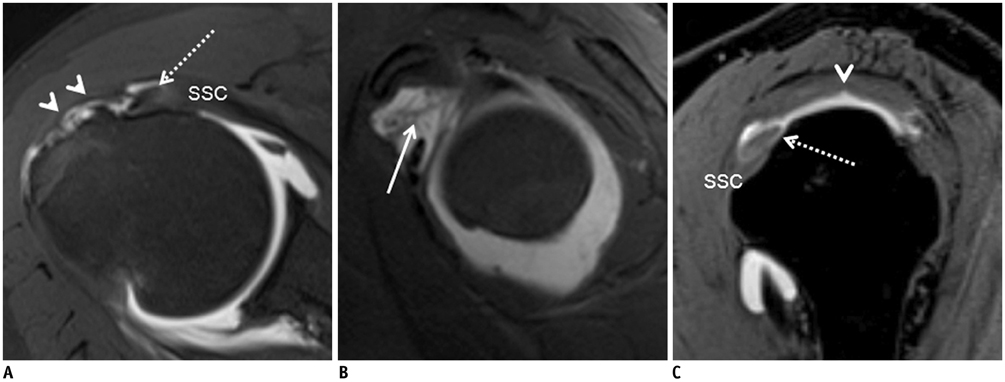
Fig. 14 Habermeyer group 2 lesion in 47-year-old woman. A. Axial fat-saturated T1-weighted MR arthrographic image shows partial articular-side supraspinatus tendon tear (white arrowheads). LHBT is slightly dislocated anteriorly (white dotted arrow). B. Oblique sagittal fat-saturated T1-weighted MR arthrographic image demonstrates fraying of SGHL (white arrow). C. Oblique sagittal fat-saturated 3D VIBE MR arthrographic image demonstrates displacement sign. LHBT (white dotted arrow) shows contact with superior border of intact subscapularis tendon (SSC) on midsection through lesser tuberosity. SGHL is invisible. Image also shows partial tear on articular-side supraspinatus tendon (white arrowhead), increased signal intensity, and diameter of LHBT (white dotted arrow). LHBT = long head of biceps tendon, SGHL = superior glenohumeral ligament, 3D VIBE = three-dimensional volumetric interpolated breath-hold examination
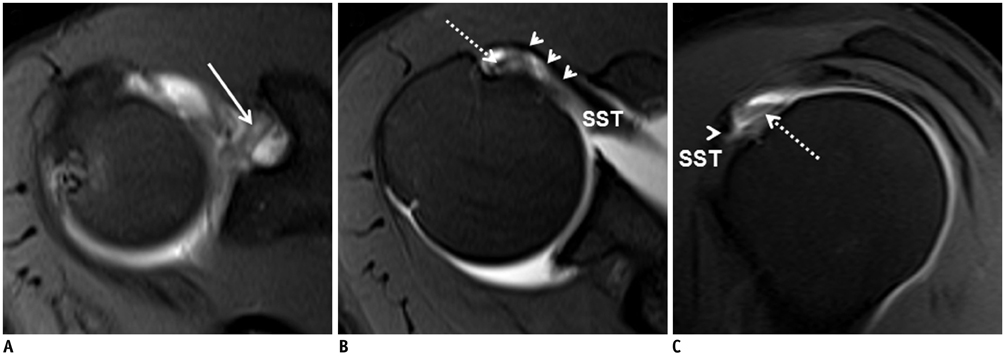
Fig. 15 Habermeyer group 3 lesion in 38-year-old woman. A, B. Consecutive axial fat-saturated T1-weighted MR arthrographic images show superior GHL lesion (white arrow) with partial tear on articular-side of subscapularis tendon (white arrowheads). LHBT (white dotted arrow) shows slight medial subluxation. C. Oblique sagittal fat-saturated T1-weighted MR arthrographic image shows contrast agent entering defect (arrowhead) of superior subscapularis tendon (SSC), consistent with partial tear. LHBT (white dotted arrow) shows contact with superior border of SSC on midsection through lesser tuberosity. LHBT = long head of biceps tendon, SST = supraspinatus tendon
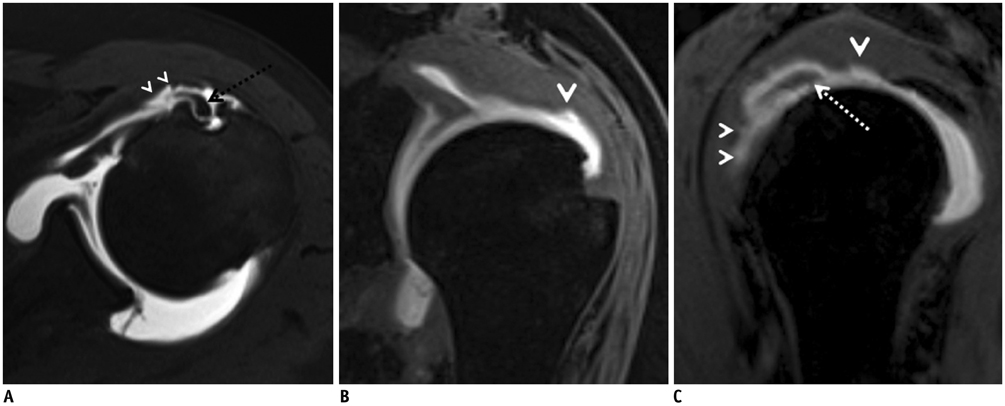
Fig. 16 Habermeyer group 4 lesion in 55-year-old man. A. Axial fat-saturated T1-weighted MR arthrographic image shows medial subluxation of LHBT (black dotted arrow) with partial tear on articularside of subscapularis tendon (white arrowheads). B. Oblique coronal fat-saturated 3D VIBE MR arthrographic image shows partial tear on articular-side of supraspinatus tendon (white arrowhead). C. Oblique sagittal fat-saturated 3D VIBE MR arthrographic image shows partial tears on articular-side of supraspinatus and subscapularis tendons. Displacement sign is shown, with LHBT (white dotted arrow) cutting into superior portion of subscapularis tendon (small white arrowheads). Image also shows partial tear on articular-side of supraspinatus tendon (big white arrowhead), increased signal intensity, and diameter of LHBT (white dotted arrow). LHBT = long head of biceps tendon, 3D VIBE = three-dimensional volumetric interpolated breath-hold examination
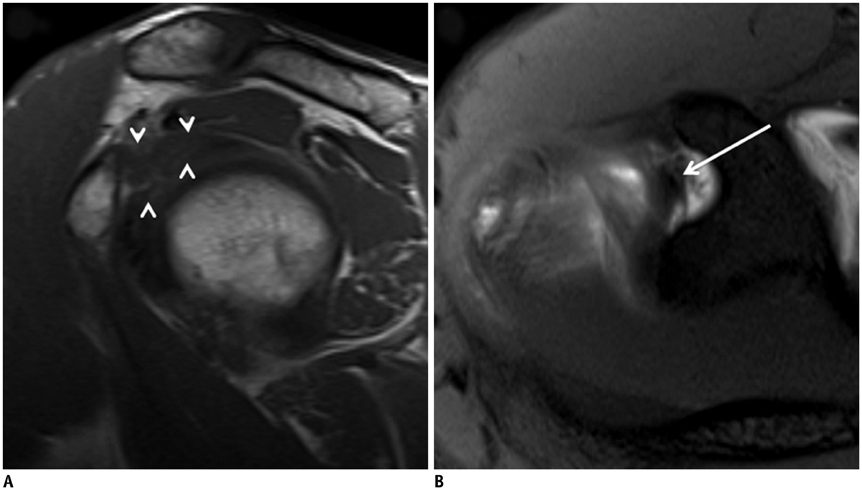
Fig. 17 Frozen shoulder of 45-year-old man. A. Oblique sagittal T1-weighted MR image shows complete obliteration of subcoracoid fat triangle (white arrowheads). B. Axial fat-saturated T1-weighted MR arthrographic image shows thickened SGHL (white arrow). SGHL = superior glenohumeral ligament
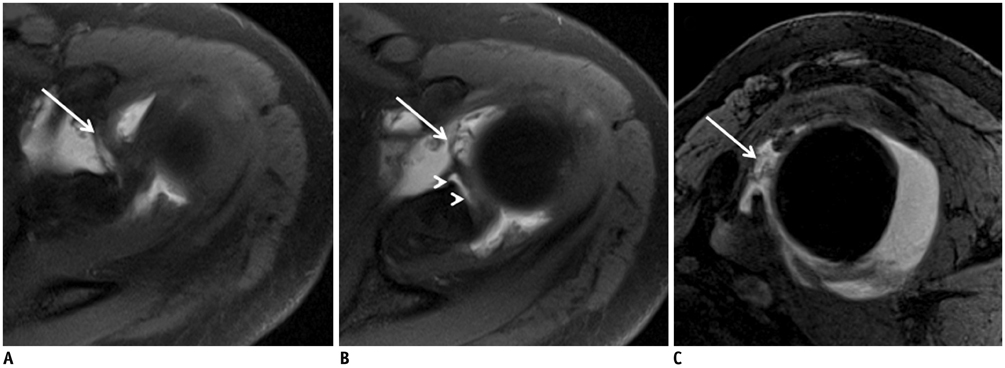
Fig. 18 Type X SLAP lesion with SGHL tear in 43-year-old man. A, B. Consecutive axial fat-saturated 3D VIBE MR arthrographic images show tears of SGHL (white arrow) and superior labrum (white arrowheads). C. Oblique sagittal fat-saturated 3D VIBE MR arthrographic image shows SGHL tear (white arrow) between subscapularis tendon and LHBT. LHBT = long head of biceps tendon, SGHL = superior glenohumeral ligament, SLAP = superior labrum anterior and posterior, 3D VIBE = three-dimensional volumetric interpolated breath-hold examination

Fig. 19 Massive anterior labral tear with SGHL tear in 36-year-old man. A. Axial fat-saturated T1-weighted MR arthrographic image shows avulsion of anteroinferior glenoid labrum (black dotted arrow) behind MGHL (black arrowhead). B. Upper section of axial fat-saturated T1-weighted MR arthrography shows SGHL tear (white arrow). C. Oblique sagittal fat-saturated 3D VIBE MR arthrographic image shows massive avulsion of anterior glenoid labrum (white dotted arrow) behind MGHL (black arrowhead). MGHL = middle glenohumeral ligament, SGHL = superior glenohumeral ligament, 3D VIBE = three-dimensional volumetric interpolated breath-hold examination
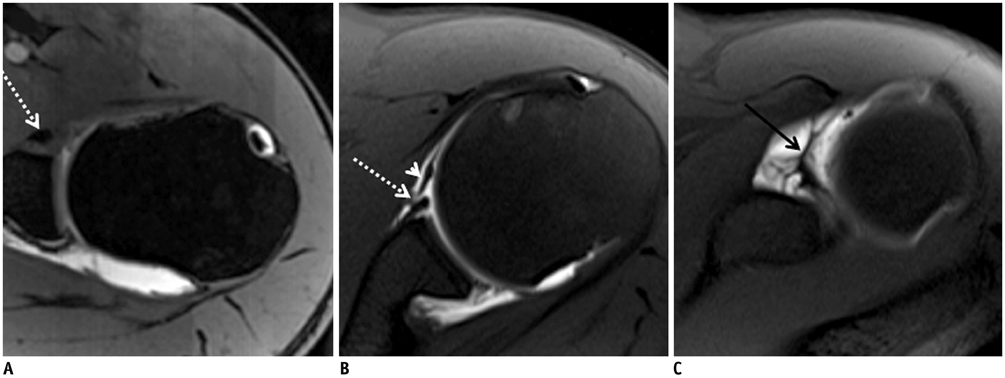
Fig. 20 Bony Bankart lesion with SGHL tear in 38-year-old woman who suffered from recurrent shoulder dislocations. A. Axial fat-saturated 3D VIBE MR arthrographic image shows classic bony Bankart lesion, with avulsion of anteroinferior glenoid bone and labrum (white dotted arrow). B. Upper section of axial fat-saturated T1-weighted MR arthrography shows avulsion of anterior glenoid labrum (white dotted arrow) behind MGHL (white arrowhead). C. Axial fat-saturated T1-weighted MR arthrographic image at level of coracoid process shows SGHL tear (black arrow). MGHL = middle glenohumeral ligament, SGHL = superior glenohumeral ligament, 3D VIBE = three-dimensional volumetric interpolated breath-hold examination

Fig. 21 Susceptibility artifacts caused by inadvertently injected air in 47-year-old man who suffered from anterosuperior shoulder pain. A. Axial fat-saturated 3D VIBE MR arthrographic image shows small air bubbles (black dotted arrows) distributed at superior part of joint cavity. Susceptibility artifacts may be more pronounced in VIBE MR arthrographic images. B. Axial fat-saturated T1-weighted MR arthrographic image at same level as VIBE sequence shows smaller air bubbles (white arrows) distributed at superior part of joint cavity. 3D VIBE = three-dimensional volumetric interpolated breath-hold examination
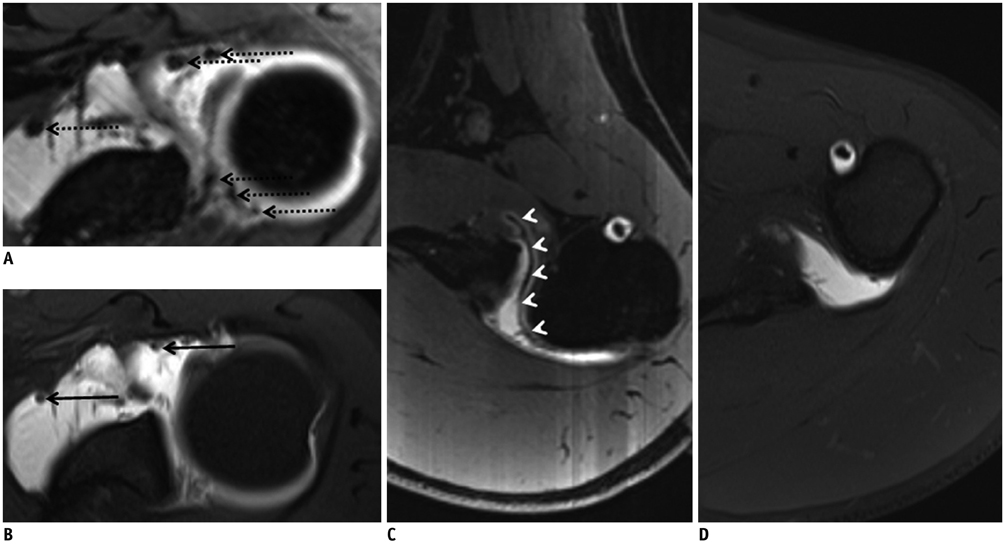
Fig. 22 Bony Bankart lesion with intraarticular blooming artifacts in 41-year-old man who suffered from shoulder dislocations. In this patient, hemosiderin deposits in synovium have been confirmed by arthroscopy. A. Axial fat-saturated 3D VIBE MR arthrographic image at level of superior glenoid shows multiple blooming artifacts (black dotted arrows) at superior part of joint cavity. B. Axial fat-saturated T1-weighted MR arthrographic image at same level as A shows smaller blooming artifacts (black arrows). C. Axial fat-saturated 3D VIBE MR arthrographic image at level of axillary recess shows synovial haemosiderin deposits (white arrowheads). D. Axial fat-saturated T1-weighted MR arthrographic image at same level as C does not show evidence of synovial haemosiderin deposits.
Reference
-
1. Bencardino JT, Beltran J. MR imaging of the glenohumeral ligaments. Magn Reson Imaging Clin N Am. 2004; 12:11–24. v2. Yang C, Goto A, Sahara W, Yoshikawa H, Sugamoto K. In vivo three-dimensional evaluation of the functional length of glenohumeral ligaments. Clin Biomech (Bristol, Avon). 2010; 25:137–141.3. Robinson G, Ho Y, Finlay K, Friedman L, Harish S. Normal anatomy and common labral lesions at MR arthrography of the shoulder. Clin Radiol. 2006; 61:805–821.4. Cooper DE, O'Brien SJ, Warren RF. Supporting layers of the glenohumeral joint. An anatomic study. Clin Orthop Relat Res. 1993; (289):144–155.5. Pouliart N, Somers K, Eid S, Gagey O. Variations in the superior capsuloligamentous complex and description of a new ligament. J Shoulder Elbow Surg. 2007; 16:821–836.6. Ogul H, Bayraktutan U, Yildirim OS, Suma S, Ozgokce M, Okur A, et al. Magnetic Resonance Arthrography of the Glenohumeral Joint: Ultrasonography-Guided Technique Using a Posterior Approach. Eurasian J Med. 2012; 44:73–78.7. Zwar RB, Read JW, Noakes JB. Sonographically guided glenohumeral joint injection. AJR Am J Roentgenol. 2004; 183:48–50.8. Souza PM, Aguiar RO, Marchiori E, Bardoe SA. Arthrography of the shoulder: a modified ultrasound guided technique of joint injection at the rotator interval. Eur J Radiol. 2010; 74:e29–e32.9. Yeh L, Kwak S, Kim YS, Pedowitz R, Trudell D, Muhle C, et al. Anterior labroligamentous structures of the glenohumeral joint: correlation of MR arthrography and anatomic dissection in cadavers. AJR Am J Roentgenol. 1998; 171:1229–1236.10. Flannigan B, Kursunoglu-Brahme S, Snyder S, Karzel R, Del Pizzo W, Resnick D. MR arthrography of the shoulder: comparison with conventional MR imaging. AJR Am J Roentgenol. 1990; 155:829–832.11. Kaplan PA, Bryans KC, Davick JP, Otte M, Stinson WW, Dussault RG. MR imaging of the normal shoulder: variants and pitfalls. Radiology. 1992; 184:519–524.12. Chung CB, Dwek JR, Cho GJ, Lektrakul N, Trudell D, Resnick D. Rotator cuff interval: evaluation with MR imaging and MR arthrography of the shoulder in 32 cadavers. J Comput Assist Tomogr. 2000; 24:738–743.13. Nakata W, Katou S, Fujita A, Nakata M, Lefor AT, Sugimoto H. Biceps pulley: normal anatomy and associated lesions at MR arthrography. Radiographics. 2011; 31:791–810.14. De Maeseneer M, Van Roy F, Lenchik L, Shahabpour M, Jacobson J, Ryu KN, et al. CT and MR arthrography of the normal and pathologic anterosuperior labrum and labral-bicipital complex. Radiographics. 2000; 20 Spec No:S67–S81.15. De Maeseneer M, Van Roy P, Shahabpour M. Normal MR imaging anatomy of the rotator cuff tendons, glenoid fossa, labrum, and ligaments of the shoulder. Radiol Clin North Am. 2006; 44:479–487. vii16. Dunham KS, Bencardino JT, Rokito AS. Anatomic variants and pitfalls of the labrum, glenoid cartilage, and glenohumeral ligaments. Magn Reson Imaging Clin N Am. 2012; 20:213–228. x17. Petchprapa CN, Beltran LS, Jazrawi LM, Kwon YW, Babb JS, Recht MP. The rotator interval: a review of anatomy, function, and normal and abnormal MRI appearance. AJR Am J Roentgenol. 2010; 195:567–576.18. Yu D, Turmezei TD, Kerslake RW. FIESTA: an MR arthrography celebration of shoulder joint anatomy, variants, and their mimics. Clin Anat. 2013; 26:213–227.19. Shankman S, Bencardino J, Beltran J. Glenohumeral instability: evaluation using MR arthrography of the shoulder. Skeletal Radiol. 1999; 28:365–382.20. Kask K, Põldoja E, Lont T, Norit R, Merila M, Busch LC, et al. Anatomy of the superior glenohumeral ligament. J Shoulder Elbow Surg. 2010; 19:908–916.21. Chandnani VP, Gagliardi JA, Murnane TG, Bradley YC, DeBerardino TA, Spaeth J, et al. Glenohumeral ligaments and shoulder capsular mechanism: evaluation with MR arthrography. Radiology. 1995; 196:27–32.22. Beltran J, Rosenberg ZS, Chandnani VP, Cuomo F, Beltran S, Rokito A. Glenohumeral instability: evaluation with MR arthrography. Radiographics. 1997; 17:657–673.23. Weishaupt D, Zanetti M, Tanner A, Gerber C, Hodler J. Lesions of the reflection pulley of the long biceps tendon. MR arthrographic findings. Invest Radiol. 1999; 34:463–469.24. Habermeyer P, Magosch P, Pritsch M, Scheibel MT, Lichtenberg S. Anterosuperior impingement of the shoulder as a result of pulley lesions: a prospective arthroscopic study. J Shoulder Elbow Surg. 2004; 13:5–12.25. Braun S, Horan MP, Elser F, Millett PJ. Lesions of the biceps pulley. Am J Sports Med. 2011; 39:790–795.26. Cooper DE, O'Brien SJ, Arnoczky SP, Warren RF. The structure and function of the coracohumeral ligament: an anatomic and microscopic study. J Shoulder Elbow Surg. 1993; 2:70–77.27. Werner A, Mueller T, Boehm D, Gohlke F. The stabilizing sling for the long head of the biceps tendon in the rotator cuff interval. A histoanatomic study. Am J Sports Med. 2000; 28:28–31.28. Schaeffeler C, Waldt S, Holzapfel K, Kirchhoff C, Jungmann PM, Wolf P, et al. Lesions of the biceps pulley: diagnostic accuracy of MR arthrography of the shoulder and evaluation of previously described and new diagnostic signs. Radiology. 2012; 264:504–513.29. Gaskill TR, Braun S, Millett PJ. Multimedia article. The rotator interval: pathology and management. Arthroscopy. 2011; 27:556–567.30. Baumann B, Genning K, Böhm D, Rolf O, Gohlke F. Arthroscopic prevalence of pulley lesions in 1007 consecutive patients. J Shoulder Elbow Surg. 2008; 17:14–20.31. Walch G, Nove-Josserand L, Levigne C, Renaud E. Tears of the supraspinatus tendon associated with "hidden" lesions of the rotator interval. J Shoulder Elbow Surg. 1994; 3:353–360.32. Bennett WF. Subscapularis, medial, and lateral head coracohumeral ligament insertion anatomy. Arthroscopic appearance and incidence of "hidden" rotator interval lesions. Arthroscopy. 2001; 17:173–180.33. Gerber C, Sebesta A. Impingement of the deep surface of the subscapularis tendon and the reflection pulley on the anterosuperior glenoid rim: a preliminary report. J Shoulder Elbow Surg. 2000; 9:483–490.34. Snyder SJ, Karzel RP, Del Pizzo W, Ferkel RD, Friedman MJ. SLAP lesions of the shoulder. Arthroscopy. 1990; 6:274–279.35. Hodler J. Technical errors in MR arthrography. Skeletal Radiol. 2008; 37:9–18.36. Gückel C, Nidecker A. The rope ladder: an uncommon artifact and potential pitfall in MR arthrography of the shoulder. AJR Am J Roentgenol. 1997; 168:947–950.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Magnetic Resonance Arthrography in the evaluation of Anterior Glenohumeral Instability
- Comparison of Non-Breath-Hold T2-weighted Turbo Spin-Echo and Three Breath-Hold T2-weighted MR Images for Detection of Focal Hepatic Lesion
- Ankle Ligaments: Comparison of MR Arthrography with Conventional MR Imaging in Amputated Feet
- Advanced Methods in Dynamic Contrast Enhanced Arterial Phase Imaging of the Liver
- Contrast-Enhanced Three-Dimensional MR Imaging Using a Volumetric Interpolated Breath-hold Examination (VIBE): Clinical Utility in the Evaluation of Renal Tumors
