Endoscopic Thyroidectomy via an Axillo-Breast Approach without Gas Insufflation for Benign Thyroid Nodules and Micropapillary Carcinomas: Preliminary Results
- Affiliations
-
- 1Department of Otorhinolaryngology, Yonsei University College of Medicine, Seoul, Korea. ywkohent@yuhs.ac
- KMID: 1727998
- DOI: http://doi.org/10.3349/ymj.2011.52.4.643
Abstract
- PURPOSE
To examine the feasibility of endoscopic thyroidectomy (ET) via an axillo-breast approach without gas insufflation for large thyroid tumors and micropapillary carcinomas.
MATERIALS AND METHODS
The patients in the benign group were separated into groups 1 (n=95, <4 cm in tumor diameter) and 2 (n=37, > or =4 cm in tumor diameter). Also, 57 patients in the micropapillary carcinoma group underwent an endoscopic hemithyroidectomy (HT) (group 3) and were compared with 60 patients who received conventional open HT (group 4). Postoperative functional outcome, local complications, surgical outcomes, and pathological outcomes were compared between the groups.
RESULTS
In the benign group, there was no significant difference in mean operating time, hospital stay, or overall perioperative complications between the two groups. In the micropapillary carcinoma group, mean operating time and hospital stay in group 3 were significantly longer than in group 4 (p=0.015 and p< or =0.001). The overall perioperative complications did not differ significantly between the groups. The postoperative cosmetic result was better in groups 1-3 (endo group) than in group 4 (open group).
CONCLUSION
ET via a gasless axillo-breast approach seems to be a safe procedure even for benign thyroid lesions > or =4 cm and micropapillary carcinomas. Although it has the advantage of better cosmetic results over open thyroidectomy, there is room for improvement in terms of lessening its invasiveness and shortening the operative time.
MeSH Terms
Figure
-
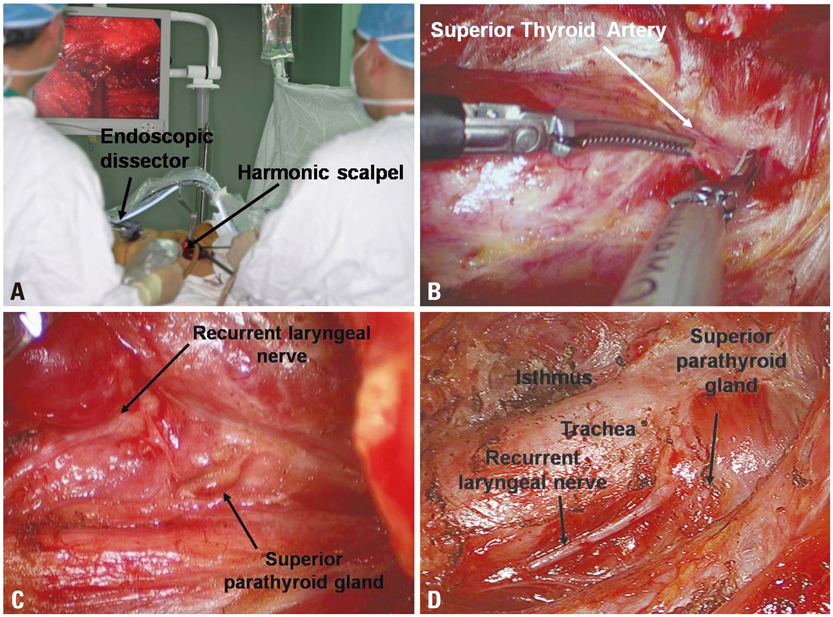
Fig. 1 Axillo-breast approach. (A) A working space is created by inserting an external retractor (Sejong Medical Corporation) through the axillary skin incision. The periareolar skin incision is used for the placement of a 12-mm trocar. (B) The superior thyroid artery (left) is easily identified and sealed off using the harmonic scalpel. (C) The left superior parathyroid gland was identified and preserved between the recurrent laryngeal nerve and common carotid artery (CCA). (D) The left endoscopic hemithyroidectomy was completed.
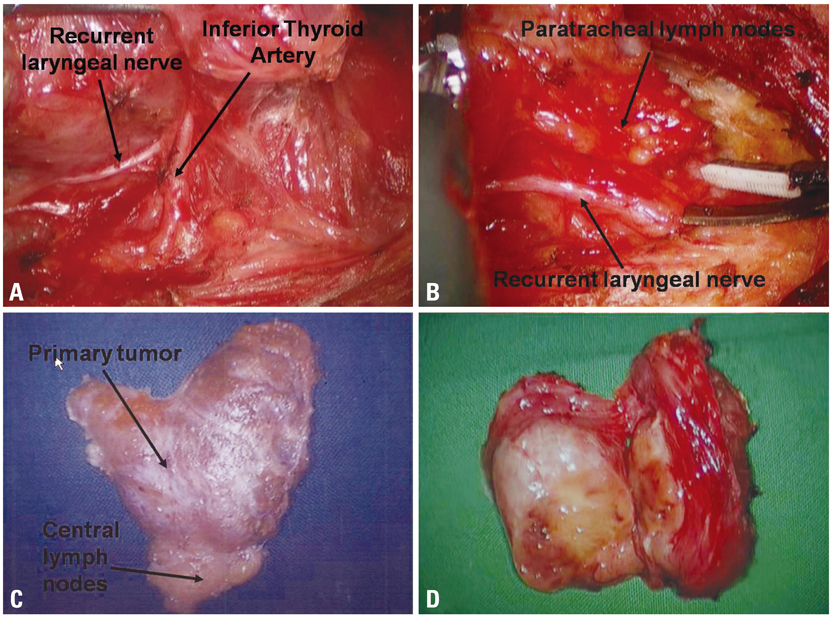
Fig. 2 Surgical procedures for the unilateral axillo-breast approach. (A) The inferior thyroid artery was identified close to the recurrent laryngeal nerve. (B) Hemithyroidectomy with paratracheal lymph node dissection is performed with careful dissection of the recurrent laryngeal nerve. (C) The left hemithyroidectomy-specimen-en bloc with ipsilateral CND is shown. (D) A specimen of large goiter resected via hemithyroidectomy (HT). The surgical specimens showed that thyroidectomy was accomplished without violation of the thyroid capsule.
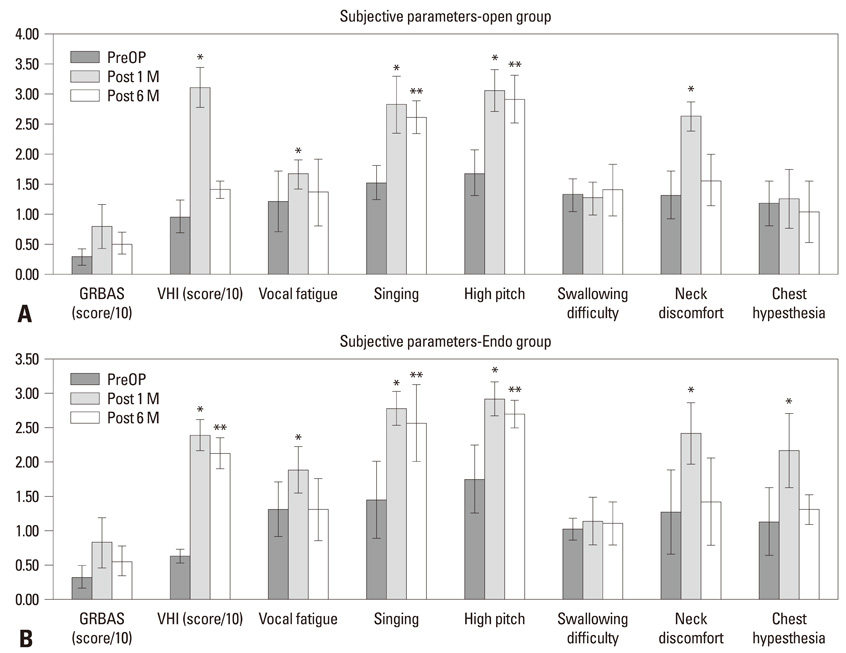
Fig. 3 Postoperative functional outcome [GRBAS scale, Voice Handicap Index (VHI)], easy fatigue during phonation, difficulty with high pitch and singing voice, hypoesthesia or paraesthesia in the neck or anterior chest wall, and swallowing difficulty were analyzed at postoperative months 1 (Post 1M) and 6 (Post 6M). * and ** Significant impairment compared to preoperative period (PreOP) (p<0.05). (A) Subjective parameters-open thyroidectomy group. (B) Subjective parameters-endoscopic thyroidectomy group.
Cited by 1 articles
-
Surgical Treatment Guidelines for Patients with Differentiated Thyroid Cancer: The Korean Association of Thyroid and Endocrine Surgeons (KATES) Guidelines Taskforce
Jin-Woo Park, Ki-Wook Chung, Ji-Sup Yun, Hyungju Kwon, Hoon Yub Kim, Kee Hyun Nam, Kyoung Sik Park, Min Ho Park, Ja Sung Bae, Hyun Jo Youn, Kyu Eun Lee, Chi Young Lim, Jin Hyang Jung, Jun-Ho Choe, , Lee Su Kim, Su Jung Lee, Jung Han Yoon
Korean J Endocr Surg. 2017;17(1):1-18. doi: 10.16956/kjes.2017.17.1.1.
Reference
-
1. Koh YW, Park JH, Kim JW, Lee SW, Choi EC. Endoscopic hemithyroidectomy with prophylactic ipsilateral central neck dissection via an unilateral axillo-breast approach without gas insufflation for unilateral micropapillary thyroid carcinoma: preliminary report. Surg Endosc. 2010. 24:188–197.
Article2. Hüscher CS, Chiodini S, Napolitano C, Recher A. Endoscopic right thyroid lobectomy. Surg Endosc. 1997. 11:877.
Article3. Yamashita H, Watanabe S, Koike E, Ohshima A, Uchino S, Kuroki S, et al. Video-assisted thyroid lobectomy through a small wound in the submandibular area. Am J Surg. 2002. 183:286–289.
Article4. Shimizu K, Akira S, Jasmi AY, Kitamura Y, Kitagawa W, Akasu H, et al. Video-assisted neck surgery: endoscopic resection of thyroid tumors with a very minimal neck wound. J Am Coll Surg. 1999. 188:697–703.
Article5. Park YL, Han WK, Bae WG. 100 cases of endoscopic thyroidectomy: breast approach. Surg Laparosc Endosc Percutan Tech. 2003. 13:20–25.6. Ohgami M, Ishii S, Arisawa Y, Ohmori T, Noga K, Furukawa T, et al. Scarless endoscopic thyroidectomy: breast approach for better cosmesis. Surg Laparosc Endosc Percutan Tech. 2000. 10:1–4.
Article7. Jung EJ, Park ST, Ha WS, Choi SK, Hong SC, Lee YJ, et al. Endoscopic thyroidectomy using a gasless axillary approach. J Laparoendosc Adv Surg Tech A. 2007. 17:21–25.
Article8. Ikeda Y, Takami H, Sasaki Y, Takayama J, Niimi M, Kan S. Comparative study of thyroidectomies. Endoscopic surgery versus conventional open surgery. Surg Endosc. 2002. 16:1741–1745.9. Kim JS, Kim KH, Ahn CH, Jeon HM, Kim EG, Jeon CS. A clinical analysis of gasless endoscopic thyroidectomy. Surg Laparosc Endosc Percutan Tech. 2001. 11:268–272.
Article10. Shimazu K, Shiba E, Tamaki Y, Takiguchi S, Taniguchi E, Ohashi S, et al. Endoscopic thyroid surgery through the axillo-bilateral-breast approach. Surg Laparosc Endosc Percutan Tech. 2003. 13:196–201.
Article11. Yeh TS, Jan YY, Hsu BR, Chen KW, Chen MF. Video-assisted endoscopic thyroidectomy. Am J Surg. 2000. 180:82–85.
Article12. Yoon JH, Park CH, Chung WY. Gasless endoscopic thyroidectomy via an axillary approach: experience of 30 cases. Surg Laparosc Endosc Percutan Tech. 2006. 16:226–231.
Article13. Chung YS, Choe JH, Kang KH, Kim SW, Chung KW, Park KS, et al. Endoscopic thyroidectomy for thyroid malignancies: comparison with conventional open thyroidectomy. World J Surg. 2007. 31:2302–2306.
Article14. Choe JH, Kim SW, Chung KW, Park KS, Han W, Noh DY, et al. Endoscopic thyroidectomy using a new bilateral axillo-breast approach. World J Surg. 2007. 31:601–606.
Article15. Bellantone R, Lombardi CP, Bossola M, Boscherini M, De Crea C, Alesina PF, et al. Video-assisted vs conventional thyroid lobectomy: a randomized trial. Arch Surg. 2002. 137:301–304.16. Henry JF, Raffaelli M, Iacobone M, Volot F. Video-assisted parathyroidectomy via the lateral approach vs conventional surgery in the treatment of sporadic primary hyperparathyroidism: results of a case-control study. Surg Endosc. 2001. 15:1116–1119.
Article17. Sakuraba M, Miyamoto H, Oh S, Shiomi K, Sonobe S, Takahashi N, et al. Video-assisted thoracoscopic lobectomy vs. conventional lobectomy via open thoracotomy in patients with clinical stage IA non-small cell lung carcinoma. Interact Cardiovasc Thorac Surg. 2007. 6:614–617.
Article18. Tschernko EM, Hofer S, Bieglmayer C, Wisser W, Haider W. Early postoperative stress: video-assisted wedge resection/lobectomy vs. conventional axillary thoracotomy. Chest. 1996. 109:1636–1642.19. Kang SW, Jeong JJ, Yun JS, Sung TY, Lee SC, Lee YS, et al. Robot-assisted endoscopic surgery for thyroid cancer: experience with the first 100 patients. Surg Endosc. 2009. 23:2399–2406.
Article20. Jeong JJ, Kang SW, Yun JS, Sung TY, Lee SC, Lee YS, et al. Comparative study of endoscopic thyroidectomy versus conventional open thyroidectomy in papillary thyroid microcarcinoma (PTMC) patients. J Surg Oncol. 2009. 100:477–480.
Article21. Ikeda Y, Takami H, Sasaki Y, Kan S, Niimi M. Endoscopic neck surgery by the axillary approach. J Am Coll Surg. 2000. 191:336–340.22. Gagner M, Inabnet WB 3rd. Endoscopic thyroidectomy for solitary thyroid nodules. Thyroid. 2001. 11:161–163.
Article23. Colonna M, Guizard AV, Schvartz C, Velten M, Raverdy N, Molinie F, et al. A time trend analysis of papillary and follicular cancers as a function of tumour size: a study of data from six cancer registries in France (1983-2000). Eur J Cancer. 2007. 43:891–900.
Article24. Koh YW, Kim JW, Lee SW, Choi EC. Endoscopic thyroidectomy via a unilateral axillo-breast approach without gas insufflation for unilateral benign thyroid lesions. Surg Endosc. 2009. 23:2053–2060.
Article25. Miyano G, Lobe TE, Wright SK. Bilateral transaxillary endoscopic total thyroidectomy. J Pediatr Surg. 2008. 43:299–303.
Article26. Rafferty M, Miller I, Timon C. Minimal incision for open thyroidectomy. Otolaryngol Head Neck Surg. 2006. 135:295–298.
Article27. Schardey HM, Schopf S, Kammal M, Barone M, Rudert W, Hernandez-Richter T, et al. Invisible scar endoscopic thyroidectomy by the dorsal approach: experimental development of a new technique with human cadavers and preliminary clinical results. Surg Endosc. 2008. 22:813–820.
Article28. Yeung GH. Endoscopic thyroid surgery today: a diversity of surgical strategies. Thyroid. 2002. 12:703–706.
Article29. Slotema ET, Sebag F, Henry JF. What is the evidence for endoscopic thyroidectomy in the management of benign thyroid disease? World J Surg. 2008. 32:1325–1332.
Article30. Inabnet WB 3rd, Jacob BP, Gagner M. Minimally invasive endoscopic thyroidectomy by a cervical approach. Surg Endosc. 2003. 17:1808–1811.
Article31. Duncan TD, Rashid QN, Speights F. Surgical excision of large multinodular goiter using an endoscopic transaxillary approach: a case report. Surg Laparosc Endosc Percutan Tech. 2008. 18:530–535.
Article32. Ruggieri M, Straniero A, Genderini M, D'Armiento M, Fumarola A, Trimboli P, et al. The size criteria in minimally invasive video-assisted thyroidectomy. BMC Surg. 2007. 7:2.
Article33. Miccoli P, Minuto MN, Ugolini C, Pisano R, Fosso A, Berti P. Minimally invasive video-assisted thyroidectomy for benign thyroid disease: an evidence-based review. World J Surg. 2008. 32:1333–1340.
Article34. Miccoli P, Berti P, Raffaelli M, Conte M, Materazzi G, Galleri D. Minimally invasive video-assisted thyroidectomy. Am J Surg. 2001. 181:567–570.
Article35. Miccoli P, Berti P, Raffaelli M, Materazzi G, Baldacci S, Rossi G. Comparison between minimally invasive video-assisted thyroidectomy and conventional thyroidectomy: a prospective randomized study. Surgery. 2001. 130:1039–1043.
Article36. Kang SW, Lee SC, Lee SH, Lee KY, Jeong JJ, Lee YS, et al. Robotic thyroid surgery using a gasless, transaxillary approach and the da Vinci S system: the operative outcomes of 338 consecutive patients. Surgery. 2009. 146:1048–1055.
Article37. Lobe TE, Wright SK, Irish MS. Novel uses of surgical robotics in head and neck surgery. J Laparoendosc Adv Surg Tech A. 2005. 15:647–652.
Article38. Gutt CN, Oniu T, Mehrabi A, Kashfi A, Schemmer P, Büchler MW. Robot-assisted abdominal surgery. Br J Surg. 2004. 91:1390–1397.
Article39. Savitt MA, Gao G, Furnary AP, Swanson J, Gately HL, Handy JR. Application of robotic-assisted techniques to the surgical evaluation and treatment of the anterior mediastinum. Ann Thorac Surg. 2005. 79:450–455.
Article40. Link RE, Bhayani SB, Kavoussi LR. A prospective comparison of robotic and laparoscopic pyeloplasty. Ann Surg. 2006. 243:486–491.
Article41. White ML, Gauger PG, Doherty GM. Central lymph node dissection in differentiated thyroid cancer. World J Surg. 2007. 31:895–904.
Article42. Shindo M, Wu JC, Park EE, Tanzella F. The importance of central compartment elective lymph node excision in the staging and treatment of papillary thyroid cancer. Arch Otolaryngol Head Neck Surg. 2006. 132:650–654.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endoscopic Removal of Parathyroid Tumors via an Unilateral Axillo-Breast Approach
- Endoscopic Hemithyroidectomy via a Unilateral Axillo-Breast Approach without Gas Insufflation in Unilateral Benign Thyroid Lesions: Preliminary Results of a Novel Approach
- Endoscopic Thyroidectomy via an Axillo-bilateral Breast Approach: 5 Years of Experience
- Nationwide Multicenter Survey for Current Status of Endoscopic Thyroidectomy in Korea
- Bilateral axillo-breast approach robotic total thyroidectomy without isthmectomy: a case report
