Using Multidetector-Row CT for the Diagnosis of Afferent Loop Syndrome Following Gastroenterostomy Reconstruction
- Affiliations
-
- 1Department of Radiology, Tri-Service General Hospital and National Defense Medical Center, Taipei, Taiwan. weichou.chang@gmail.com
- 2Department of Radiology, Hualien Armed Forces General Hospital, Hualien, Taiwan.
- 3Division of General Surgery, Department of Surgery, Tri-Service General Hospital and National Defense Medical Center, Taipei, Taiwan.
- 4Department of Healthcare Administration, Asia University, Taichung, Taiwan.
- KMID: 1727988
- DOI: http://doi.org/10.3349/ymj.2011.52.4.574
Abstract
- PURPOSE
To assess the clinical manifestations and multidetector-row computed tomography (MDCT) findings of afferent loop syndrome (ALS) and to determine the role of MDCT on treatment decisions.
MATERIALS AND METHODS
From January 2004 to December 2008, 1,100 patients had undergone gastroenterostomy reconstruction in our institution. Of these, 22 (2%) patients were diagnosed as ALS after surgery that included Roux-en-Y gastroenterotomy (n=9), Billroth-II gastrojejunostomy (n=7), and Whipple's operation (n=6). Clinical manifestations and MDCT features of these patients were recorded and statistically analyzed. The presumed etiologies of obstruction shown on the MDCT were correlated with clinical information and confirmed by surgery or endoscopic biopsy.
RESULTS
The most common clinical symptom was acute abdominal pain, presenting in 18 patients (82%). We found that a fluid-filled C-shaped afferent loop in combination with valvulae conniventes projecting into the lumen was the most common MDCT features of ALS. Malignant causes of ALS, such as local recurrence and carcinomatosis, are the most common etiologies of obstruction. These etiologies and associated complications can be predicted 100% by MDCT.
CONCLUSION
Our results suggest that MDCT is a reliable modality for assessing the etiologies of ALS and guiding treatment decisions.
Keyword
MeSH Terms
Figure
-
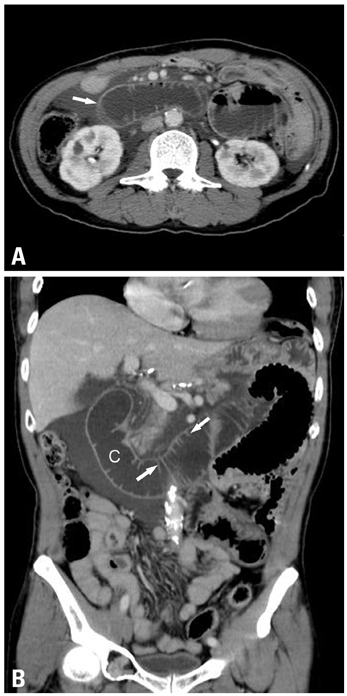
Fig. 1 Afferent loop obstruction in a 62-year-old man after Roux-en-Y gastroenterotomy. (A) Axial plane of MDCT shows a dilated fluid-filled afferent loop (arrow) located at the mid-abdomen and crossing between the aorta and superior mesenteric artery. (B) Coronal plane of MDCT reveals the configuration of the afferent loop to be of a "C" character (C). Keyboard sign (arrows) is also clearly demonstrated. Focal bowel thickening at the anastomostic region is present, suggesting local recurrence. Endoscopic biopsy confirmed the MDCT diagnosis of local recurrence.
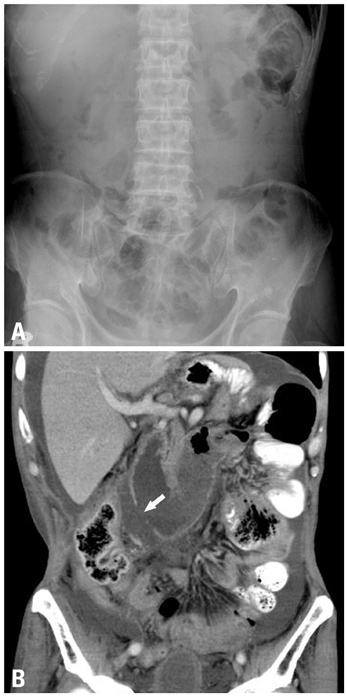
Fig. 2 Afferent loop obstruction in a 58-year-old man after Roux-en-Y gastroenterotomy. (A) Abdominal radiograph shows no remarkable findings. There is no evidence of intestinal obstruction or abnormal free extraluminal air accumulation. (B) Coronal plane of MDCT reveals perforation (arrow) of the dilated fluid-filled afferent loop. The C-loop appearance is well demonstrated, but the keyboard sign is not visualized. There is no focal bowel wall thickening or mass lesion at the anastomosis. Massive ascites and peritoneal enhancement are present, suggesting carcinomatosis. The second operation confirmed the MDCT diagnosis of carcinomatosis.
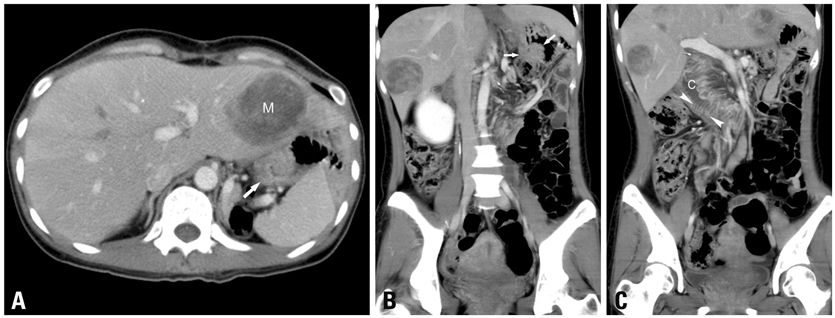
Fig. 3 Afferent loop obstruction in a 35-year-old woman after Billroth-II gastrojejunostomy. (A) Axial plane of MDCT shows bowel wall thickening (arrow) instead of appreciable lobulated mass-like lesion at the anastomosis area. (M: liver metastasis) (B) Coronal plane of MDCT clearly demonstrates the lobulated contour of soft-tissue mass (arrows) at the anastomosis, suggesting local recurrence. (C) Another coronal plane of MDCT demonstrates the fluid-filled C-shaped afferent loop (C), in combination with valvulae conniventes projecting into the lumen (arrowheads). This MDCT finding is highly suggestive of bowel obstruction. The endoscopic biopsy confirmed the MDCT diagnosis of local recurrence inducing afferent loop syndrome. MDCT, multidetector-row computed tomography.
Reference
-
1. Gayer G, Barsuk D, Hertz M, Apter S, Zissin R. CT diagnosis of afferent loop syndrome. Clin Radiol. 2002. 57:835–839.
Article2. Kim HC, Han JK, Kim KW, Kim YH, Yang HK, Kim SH, et al. Afferent loop obstruction after gastric cancer surgery: helical CT findings. Abdom Imaging. 2003. 28:624–630.
Article3. Yaghmai V, Nikolaidis P, Hammond NA, Petrovic B, Gore RM, Miller FH. Multidetector-row computed tomography diagnosis of small bowel obstruction: can coronal reformations replace axial images? Emerg Radiol. 2006. 13:69–72.
Article4. Perret RS, Sloop GD, Borne JA. Common bile duct measurements in an elderly population. J Ultrasound Med. 2000. 19:727–730.
Article5. Berland LL, Lawson TL, Foley WD, Greenen JE, Stewart ET. Computed tomography of the normal and abnormal pancreatic duct: correlation with pancreatic ductography. Radiology. 1981. 141:715–724.
Article6. Dorfman RE, Alpern MB, Gross BH, Sandler MA. Upper abdominal lymph nodes: criteria for normal size determined with CT. Radiology. 1991. 180:319–322.
Article7. Ha HK, Kim HH, Kim HS, Lee MH, Kim KT, Shinn KS. Local recurrence after surgery for gastric carcinoma: CT findings. AJR Am J Roentgenol. 1993. 161:975–977.
Article8. Maglinte DD, Gage SN, Harmon BH, Kelvin FM, Hage JP, Chua GT, et al. Obstruction of the small intestine: accuracy and role of CT in diagnosis. Radiology. 1993. 188:61–64.
Article9. Blachar A, Federle MP, Dodson SF. Internal hernia: clinical and imaging findings in 17 patients with emphasis on CT criteria. Radiology. 2001. 218:68–74.
Article10. Jordan GL Jr. Surgical management of postgastrectomy problems. Arch Surg. 1971. 102:251–259.
Article11. Iwahashi M, Nakamori M, Nakamura M, Naka T, Ojima T, Iida T, et al. Evaluation of double tract reconstruction after total gastrectomy in patients with gastric cancer: prospective randomized controlled trial. World J Surg. 2009. 33:1882–1888.
Article12. Hoya Y, Mitsumori N, Yanaga K. The advantages and disadvantages of a Roux-en-Y reconstruction after a distal gastrectomy for gastric cancer. Surg Today. 2009. 39:647–651.
Article13. Wise SW. Case 24: Afferent loop syndrome. Radiology. 2000. 216:142–145.
Article14. Zissin R, Hertz M, Paran H, Osadchy A, Gayer G. Computed tomographic features of afferent loop syndrome: pictorial essay. Can Assoc Radiol J. 2005. 56:72–78.15. Beveridge CJ, Zammit-Maempel I. Afferent loop obstruction: CT appearances of an unusual cause of acute pancreatitis. Clin Radiol. 1999. 54:188–189.
Article16. Doherty M, Perret RS. Case 1: Afferent loop syndrome. AJR Am J Roentgenol. 1998. 171:852856–857.
Article17. Kuwabara Y, Nishitani H, Numaguchi Y, Kamoi I, Matsuura K, Saito S. Afferent loop syndrome. J Comput Assist Tomogr. 1980. 4:687–689.
Article18. Pannu HK, Bristow RE, Montz FJ, Fishman EK. Multidetector CT of peritoneal carcinomatosis from ovarian cancer. Radiographics. 2003. 23:687–701.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Afferent loop syndrome: role of sonography and CT
- Acute Abdomen Caused by Complicated Afferent Loop Syndrome after Gastrectomy
- CT appearance of afferent loop syndrome: a case report
- A Case of Afferent Loop Syndrome Treated by Endoscopic Drainage Procedure using Nasogastric Tube
- A Case of Afferent Loop Syndrome with Acute Cholangitis Developed after Percutaneous Transhepatic Cholangioscopic Lithotripsy for Treatment of Choledocholithiasis in a Patient Who Underwent Billroth II Gastrectomy
