Female Longitudinal Anal Muscles or Conjoint Longitudinal Coats Extend into the Subcutaneous Tissue along the Vaginal Vestibule: A Histological Study Using Human Fetuses
- Affiliations
-
- 1Division of Colon and Rectal Surgery, Shizuoka Cancer Center Hospital, Shizuoka, Japan. y.kinugasa@scchr.jp
- 2Arakawa Clinic of Proctology, Tokyo, Japan.
- 3Department of Anatomy, Akita University School of Medicine, Akita, Japan.
- 4Department of Anatomy and Embryology II, Faculty of Medicine, Complutense University, Madrid, Spain.
- 5Division of Internal Medicine, Iwamizawa Kojin-Kai Hospital, Iwamizawa, Japan.
- 6Department of Surgical Oncology, Graduate School, Tokyo Dental and Medical University, Tokyo, Japan.
- KMID: 1727897
- DOI: http://doi.org/10.3349/ymj.2013.54.3.778
Abstract
- PURPOSE
It is still unclear whether the longitudinal anal muscles or conjoint longitudinal coats (CLCs) are attached to the vagina, although such an attachment, if present, would appear to make an important contribution to the integrated supportive system of the female pelvic floor.
MATERIALS AND METHODS
Using immunohistochemistry for smooth muscle actin, we examined semiserial frontal sections of 1) eleven female late-stage fetuses at 28-37 weeks of gestation, 2) two female middle-stage fetus (2 specimens at 13 weeks), and, 3) six male fetuses at 12 and 37 weeks as a comparison of the morphology.
RESULTS
In late-stage female fetuses, the CLCs consistently (11/11) extended into the subcutaneous tissue along the vaginal vestibule on the anterior side of the external anal sphincter. Lateral to the CLCs, the external anal sphincter also extended anteriorly toward the vaginal side walls. The anterior part of the CLCs originated from the perimysium of the levator ani muscle without any contribution of the rectal longitudinal muscle layer. However, in 2 female middle-stage fetuses, smooth muscles along the vestibulum extended superiorly toward the levetor ani sling. In male fetuses, the CLCs were separated from another subcutaneous smooth muscle along the scrotal raphe (posterior parts of the dartos layer) by fatty tissue.
CONCLUSION
In terms of topographical anatomy, the female anterior CLCs are likely to correspond to the lateral extension of the perineal body (a bulky subcutaneous smooth muscle mass present in adult women), supporting the vaginal vestibule by transmission of force from the levator ani.
MeSH Terms
Figure
-
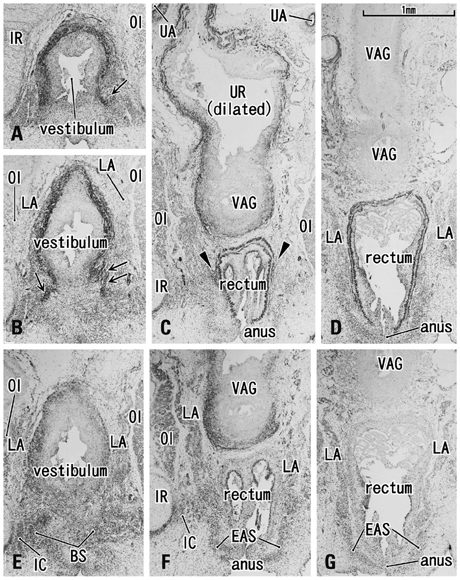
Fig. 1 Developing vaginal vestibulum accompanies smooth muscle coat at 13 weeks. Frontal sections. Panels A-D are immunohistochemistry for smooth muscle actin while panels E-G are for striated muscle myosin. Panels B and E (C and F, D and G) show the near sections. Panel A (or panel D) is the most anterior side (or posterior side) in the figure. Intervals between panels are 0.5 mm (A-B, B-C) and 0.6 mm (C-D), respectively. The developing vestibulum accopanies a smooth muscle cost and it issues muscle fibers superiorly (arrows in panels A and B). Likewise, a few smooth muscles extend from the rectum (arrowheads in panel C). The urethra (UR) or urogenital sinus is dilated and surrounded by smooth muscle layer (panel C). In contrast, most or upper parts of the vagina do not accompany smooth muscles (panel D). The striated muscle immunohistochemistry (panels E and F) displays a close relation between the bulbospongiosus (BS) and the external anal sphincter (EAS). IC, ischiocavernosus muscle; IR, ischial ramus of the pelvis; LA, levator ani; OI, obturator internus muscle; VAG, vagina.
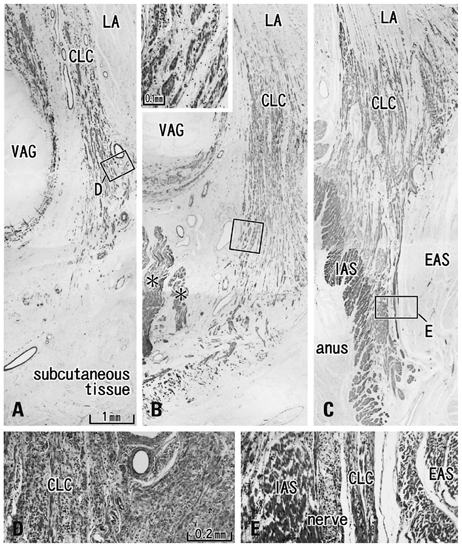
Fig. 2 Longitudinal anal muscles in a female 28-week fetus. Frontal sections. Smooth muscle actin immunohistochemistry and HE staining. Panel A (or Panel C) is the most anterior (or posterior) in the figure. Intervals between panels are 3.0 mm (A-B) and 4.5 mm (B-C), respectively. Panel D (or Panel E) is a higher magnification view of a square in panel A (or panel C). An insert at the top of panel B is also a higher magnification view corresponding to a square in the panel. The conjoint longitudinal coat (CLC) originates from the perimysium of the levator ani (LA) and insert into the subcutaneous tissue (panels A and B) or on the external and internal anal sphincters (EAS, IAS; panel C). Asterisks in panel B indicate the most anterior part of the longitudinal muscle layer of the anal canal. VAG, the most posterior part of the vagina. In HE staining (panels D and E, insert of panel B), each fiber of smooth muscle bundles (i.e., CLC or IAS) carries an irregular surface similar to a feather in contrast to a smooth surface of the striated muscle (i.e., EAS). HE, hematoxylin and eosin; VAG, vagina.
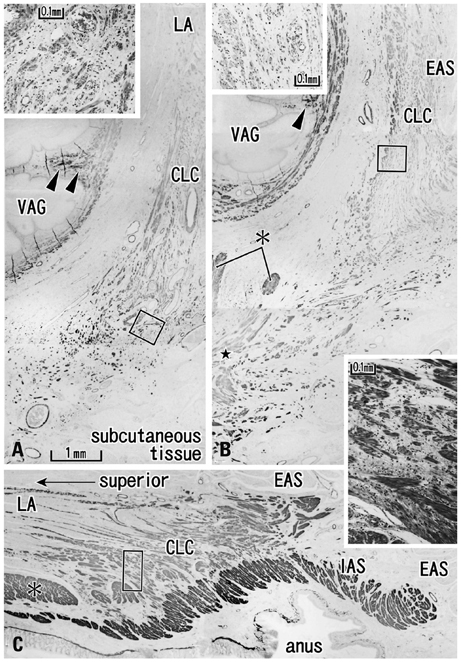
Fig. 3 Longitudinal anal muscles in a female 37-week fetus. Frontal sections. Smooth muscle actin immunohistochemistry and HE staining. Panel A (or Panel C) is the most anterior (or posterior) in the figure. The supero-inferior axis of panel C is different from panels A and B. Intervals between panels are 4.0 mm (A-B) and 6.0 mm (B-C), respectively. Inserts at the top of panels A and B are a higher magnification view corresponding to a square in the panel A or B, respectively. Another insert between panels B and C displays a square in panel C. The morphology of the conjoint longitudinal coat (CLC) is similar to that shown in Fig. 3. However, they provided thick bundles or a mass (star in panel B) in the immediately anterior side of the longitudinal muscle layer (asterisk in panel B) of the anal canal. Arrowheads indicate smooth muscles in the folds of the vagina. In HE staining (an insert for panel C), each fiber of smooth muscle bundles carries an irregular surface in contrast to a smooth surface of the striated muscle. EAS, external anal sphincter; IAS, internal anal sphincter; LA, levator ani; VAG, vagina; HE, hematoxylin and eosin.
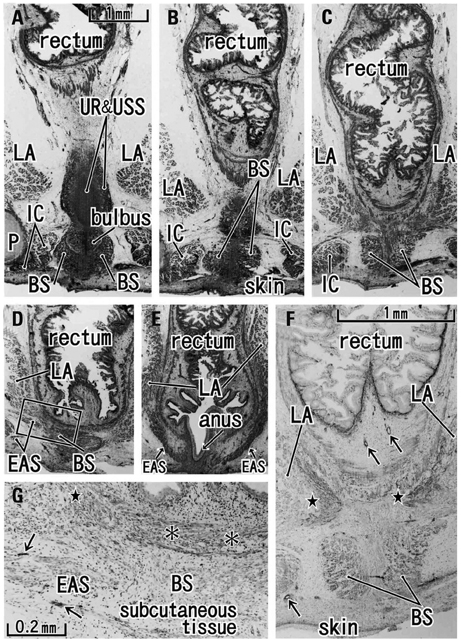
Fig. 4 Smooth muscle distribution along the male rectum at 12 weeks. Frontal sections. HE staining (panels A-E) and immunohistochemistry for alpha smooth muscle actin (panels F and G). Panel A (or Panel E) is the most anterior (or posterior) side in the figure. Intervals between panels are 0.2 mm (A-B), 0.3 mm (B-C), 0.4 mm (C-D) and 0.6 mm (D-E), respectively. Panel F (or G) is a higher magnification view of the lower part of panel C (or a square in panel D). Panel A includes the posterior margin of the urethra and urethral striated sphincter (UR&USS). The bulbospongiosus (BS) becomes smaller in the more posterior section (from panel A to D) and, in panels D and G, it shows the close relation with the external anal sphincter (EAS). Panels F and G display a smooth muscle mass (stars) at the inferomedial edge of the levator ani (LA) muscle, but the smooth muscles do not extend into the subcutaneous tissue. Asterisks in panel G indicate the smooth muscle layer in the rectal wall. The endothelium of the artery and vein (arrows in panels F and G) is also positive in the immunohistochemistry. bulbus, bulbus penis; P, pubis; IC, ischiocavernosus muscle; HE, hematoxylin and eosin.
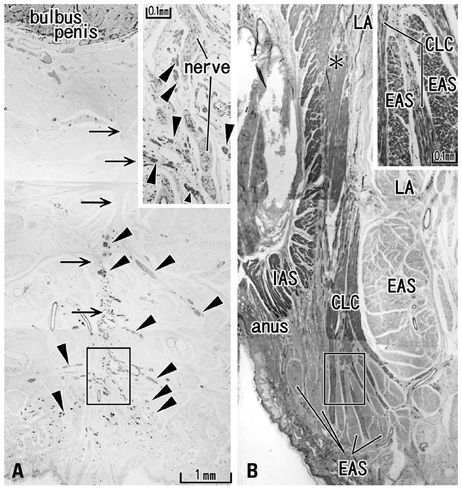
Fig. 5 Longitudinal anal muscles in a male 37-week fetus. Frontal sections. Smooth muscle actin immunohistochemistry and HE staining. Panel A, including the most posterior part of the scrotal raphe, is 5 mm anterior to panel B showing the anterolateral wall of the anus. Inserts at the top of panels A and B are a higher magnification view corresponding to a square in the panel A or B, respectively. Panel A displays subcutaneous smooth muscles (arrowheads) along and near the scrotal raphe (arrows). These smooth muscles are separated from the conjoint longitudinal coat (CLC in panel B) by the fatty tissue. The longitudinal anal muscles insert into the external anal sphincter (EAS), not into the internal sphincter (IAS). Asterisk in panel B indicates the longitudinal muscle layer of the rectum. A dark color in parts of the EAS is due to non-specific staining in immunohistochemsitry. LA, levator ani.
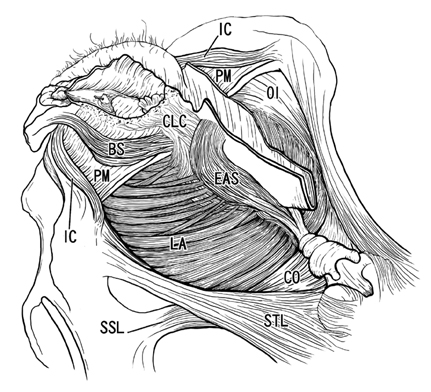
Fig. 6 A schematic representation of the female longitudinal anal muscles extending toward the vaginal vestibule. Posterosuperior view after complete dissection of the ischiorectal fossa. The present observations of the fetal conjoint longitudinal coat (CLC) are interposed onto the adult morphology. The CLC originates from the muscle associated connective tissues of the levator ani (LA) and extends antero-inferiorly into the subcutaneous tissue along and around the vaginal vestibule. These smooth muscles cross in the superficial or inferior side of the bulbospongiosus (BS). In accordance with the CLC, the external anal sphincter (EAS) also reaches the anterior site near the vaginal side walls, but we are unable to draw the morphology because of limitation of drawing skills. CO, coccygeus muscle; IC, ischiocavernosus muscle; OI, obturator internus muscle; PM, perineal membrane; SSL, sacrospinal ligament; STL, sacrotuberous ligament.
Reference
-
1. Macchi V, Porzionato A, Stecco C, Vigato E, Parenti A, De Caro R. Histo-topographic study of the longitudinal anal muscle. Clin Anat. 2008. 21:447–452.
Article2. Shafik A. New concept of the anatomy of the anal sphincter mechanism and the physiology of defecation. II. Anatomy of the levator ani muscle with special reference to puborectalis. Invest Urol. 1975. 13:175–182.3. Borley NR. Standring S, editor. Anal canal. Gray's Anatomy. 2008. 40th ed. London: Elsevier Churchill Linvingstone;1155–1160.4. Arakawa T, Murakami G, Nakajima F, Matsubara A, Ohtsuka A, Goto T, et al. Morphologies of the interfaces between the levator ani muscle and pelvic viscera, with special reference to muscle insertion into the anorectum in elderly Japanese. Anat Sci Int. 2004. 79:72–81.
Article5. Murakami G, Nakajima F, Sato TJ, Tsugane MH, Taguchi K, Tsukamoto T. Individual variations in aging of the male urethral rhabdosphincter in Japanese. Clin Anat. 2002. 15:241–252.
Article6. Hirata E, Fujiwara H, Hayashi S, Ohtsuka A, Abe S, Murakami G, et al. Intergender differences in histological architecture of the fascia pelvis parietalis: a cadaveric study. Clin Anat. 2011. 24:469–477.
Article7. Brooks JD, Eggener SE, Chao WM. Anatomy of the rectourethralis muscle. Eur Urol. 2002. 41:94–100.
Article8. Porzionato A, Macchi V, Gardi M, Parenti A, De Caro R. Histotopographic study of the rectourethralis muscle. Clin Anat. 2005. 18:510–517.
Article9. Matsubara A, Murakami G, Arakawa T, Yasumoto H, Mutaguchi K, Akita K, et al. Topographic anatomy of the male perineal structures with special reference to perineal approaches for radical prostatectomy. Int J Urol. 2003. 10:141–148.
Article10. Uchimoto K, Murakami G, Kinugasa Y, Arakawa T, Matsubara A, Nakajima Y. Rectourethralis muscle and pitfalls of anterior perineal dissection in abdominoperineal resection and intersphincteric resection for rectal cancer. Anat Sci Int. 2007. 82:8–15.
Article11. Petros P. The female pelvic floor. 2004. Heidelberg: Springer.12. Hayashi S, Murakami G, Ohtsuka A, Itoh M, Nakano T, Fukuzawa Y. Connective tissue configuration in the human liver hilar region with special reference to the liver capsule and vascular sheath. J Hepatobiliary Pancreat Surg. 2008. 15:640–647.
Article13. Miyake N, Hayashi S, Kawase T, Cho BH, Murakami G, Fujimiya M, et al. Fetal anatomy of the human carotid sheath and structures in and around it. Anat Rec (Hoboken). 2010. 293:438–445.
Article14. Soga H, Nagata I, Murakami G, Yajima T, Takenaka A, Fujisawa M, et al. A histotopographic study of the perineal body in elderly women: the surgical applicability of novel histological findings. Int Urogynecol J Pelvic Floor Dysfunct. 2007. 18:1423–1430.
Article15. DeLancey JO. Structural anatomy of the posterior pelvic compartment as it relates to rectocele. Am J Obstet Gynecol. 1999. 180:815–823.
Article16. Kato M, Matsubara A, Murakami G, Abe S, Ide Y, Sato I, et al. Female perineal membrane: a study using pelvic floor semiserial sections from elderly nulliparous and multiparous women. Int Urogynecol J Pelvic Floor Dysfunct. 2008. 19:1663–1670.
Article17. van der Putte SC. The devlopment of the perineum in the human. A comprehensive histological study with a special reference to the role of the stromal components. Adv Anat Embryol Cell Biol. 2005. 177:1–131.18. Murphy F, Puri P, Hutson JM, Holschneider AM. Holschneider AM, Hutson JM, editors. Incidence and frequency of different types, and classification of anorectal malformations. Anorectal Malformations in Children. 2006. 40th ed. Berlin Heidelberg: Springer;163–184.
Article19. Stephens FD. Holschneider AM, Hutson JM, editors. Photographic album of anorectal malformations and the sphincter muscles. Anorectal Malformations in Children. 2006. 40th ed. Berlin Heidelberg: Springer;87–142.20. van der Putte SC. The development of the human anorectum. Anat Rec (Hoboken). 2009. 292:951–954.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Perineal raphe with special reference to its extension to the anus: a histological study using human fetuses
- Reappraisal of intergender differences in the urethral striated sphincter explains why a completely circular arrangement is difficult in females: a histological study using human fetuses
- Development and growth of the temporal fascia: a histological study using human fetuses
- A Case of Retinoblastoma and Coats' Disease in the Same eye: A Clinicopathologic Report
- Anococcygeal Raphe Revisited: A Histological Study Using Mid-Term Human Fetuses and Elderly Cadavers
