J Korean Med Sci.
2006 Dec;21(6):1133-1135. 10.3346/jkms.2006.21.6.1133.
Tethered Spinal Cord with Double Spinal Lipomas
- Affiliations
-
- 1Department of Neurosurgery, Ajou University, School of Medicine, San 5, Wonchon-dong, Youngtong-gu, Suwon, Korea. ee80@ajou.ac.kr
- KMID: 1713135
- DOI: http://doi.org/10.3346/jkms.2006.21.6.1133
Abstract
- Although lumbosacral lipoma is reported to occur in 4-8 of 100,000 patients, and 66% of lipomyelomeningoceles in young patients are accompanied by hypertrophic filum terminale, it is very rare to find two isolated spinal lipomas simultaneously. A 3 month-old baby girl was admitted to the hospital for a protruding, non-tender, soft, subcutaneous 2.5 cm mass of the lumbosacral area that had been present since birth. Simple radiography showed a spinal posterior arch defect from L3 to L5, and magnetic resonance imaging (MRI) demonstrated two isolated spinal lipomas, a transitional type from L3 to L5, and a terminal type below S1 without dural defect. The cornus medullaris was severely tethered descending to the S1, but there was no cerebellar or brain stem herniation on the MRI. We suggest that the presence of a combined spinal lipoma should be a point for careful differentiation in an infant with spinal lipoma.
MeSH Terms
Figure
-
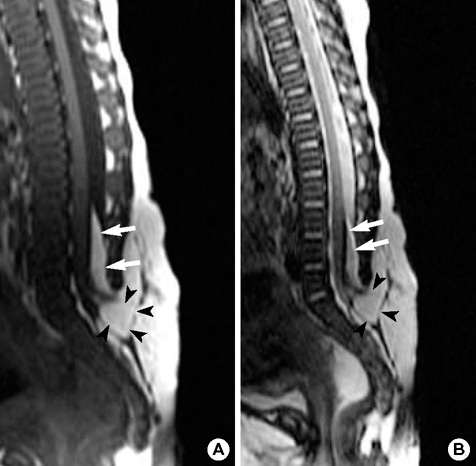
Fig. 1 Initial preoperative spine MR of T1-weighted (A) and T2-weighted images (B) shows tethered cornus medullaris to the level of sacrum and two isolated lipomyelomeningoceles, a transitional type from L3 to L5 (arrows), and a terminal type below S1 (arrow heads).

Fig. 2 (A) After incision of the dura of L2 to S1, the normal cord (arrows) and transitional type spinal lipoma (arrow heads) are exposed. (B) Another terminal type spinal lipoma (arrow heads) was exposed and removed from the filum terminale (black arrow) after upper transitional type spinal lipoma was detethered and dissected (white arrows).
Reference
-
1. Bruce DA, Schut L. Spinal lipomas in infancy and childhood. Childs Brain. 1979. 5:192–203.
Article2. Hoffman HJ, Taecholarn C, Hendrick EB, Humphreys RP. Management of lipomyelomeningoceles. Experience at the Hospital for Sick Children Toronto. J Neurosurg. 1985. 62:1–8.3. Xenos C, Sgouros S, Walsh R, Hockley A. Spinal lipomas in children. Pediatr Neurosurg. 2000. 32:295–307.
Article4. Lee JH, Shin KM, Kim MH, Song JH, Park HK, Kim SH, Park DB. Lipomyelomeningocele: Clinical analysis of 14 cases. J Korean Neurosurg Soc. 1996. 25:1196–1201.5. Byrne RW, Hayes EA, George TM, McLone DG. Operative resection of 100 spinal lipomas in infants less than 1 year of age. Pediatr Neurosurg. 1995. 23:182–187.
Article6. McLone DG, Naidich TP. Laser resection of fifty spinal lipomas. Neurosurgery. 1986. 18:611–615.
Article7. Arai H, Sato K, Okuda O, Miyajima M, Hishii M, Nakanishi H, Ishii H. Surgical experience of 120 patients with lumbosacral lipomas. Acta Neurochir (Wien). 2001. 143:857–864.
Article8. Calenbergh FV, Vanvolsem S, Verpoorten C, Lagae L, Casaer P, Plets C. Results after surgery for lumbosacral lipoma: the significance of early and late worsening. Childs Nerv Syst. 1999. 15:439–443.9. Catala M. Embryogenesis; Why do we need a new explanation for the emergence of spinal bifida with lipoma? Childs Nerv Syst. 1999. 13:336–340.10. Muraszko K, Youkilis A. Intramedullary spinal tumors of disordered embryogenesis. J Neurooncol. 2000. 47:271–281.11. French BN. Youmans JR, editor. Midline fusion defects and defects of formation. Neurological surgery. 1990. vol 2:3rd ed. Philadelphia: WB Saunders;1081–1235.12. Chapman PH, Davis KR. Surgical treatment of spinal lipomas in childhood. Pediatr Neurosurg. 1993. 19:267–275.
Article13. Chapman PH. Congenital intraspinal lipomas. Anatomic considerations and surgical treatment. Childs Brain. 1982. 9:37–47.14. Kang JK, Lee KS, Jeun SS, Lee IW, Kim MC. Role of surgery for maintaining urological function and prevention of retethering in the treatment of lipomeningomyelocele; experience recorded in 75 lipomeningomyelocele patients. Childs Nerv Syst. 2003. 19:23–29.
Article15. Pierre-Kahn A, Zerah M, Renier D, Cinalli G, Sainte-Rose C, Lellouch-Tubiana A, Brunelle F, Le Merrer M, Giudicelli Y, Pichon J, Kleinknecht B, Nataf F. Congenital lumbosacral lipomas. Childs Nerv Syst. 1997. 13:298–334.
Article16. Bailey IC. Double meningocele. Arch Dis Child. 1973. 46:549–550.
Article17. Etus V, Ilbay K, Akansel G, Ceylan S, Ceylan S. Double myelomeningocele in a neonate: Case report and review of the literature. Clin Neurol Neurosurg. 2006. 108:595–600.
Article18. Richards TA, Kortesis BG, Glazier S, Argenta LC, David LR. Double myelomeningocele: case report and review. Br J Plast Surg. 2003. 56:306–308.
Article19. Durmaz R, Arslantas A, Ozon YH, Tel E. Double meningocele. Case report. Turk J Pediatr. 2000. 42:331–333.20. Endo T, Yoshida Y, Shirane R, Yoshimoto T. Tethered spinal cord with double lipomas. J Neurosurg. 2001. 95:277.
Article21. Gorey MT, Naidich TP, McLone DG. Double discontinuous lippomyelomeningocele: CT findings. J Comput Assist Tomogr. 1985. 9:584–591.22. Pathl R, Killey M, Sage M. Isolated spinal cord lipoma. J Clin Neurosci. 2003. 10:692–694.23. Walsh JW, Markesbery WR. Histological features of congenital lipoma of the lower spinal cord. J Neurosurg. 1980. 52:564–569.24. Li YC, Shin SH, Cho BK, Lee MS, Lee YJ, Hong SK, Wang KC. Pathogenesis of lumbosacral lipoma: A test of the 'premature dysjunction' theory. Pediatr Neurosurg. 2001. 34:124–130.
Article25. Park SH, Huh JS, Cho KH, Shin YS, Kim SH, Ahn YH, Cho KG, Yoon SH. Teratoma developed in human tail lipoma. Pediatr Neurosurg. 2005. 41:158–161.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Nerve injury in an undiagnosed adult tethered cord syndrome patients following spinal anesthesia: A case report
- Intramedullary Spinal Cord Lipoma without Spinal Dysraphism
- Spinal Dysraphism and Tethered Cord Syndrome
- Tethered Cord Syndrome in Spina Bifida Occulta: A Case Report
- A Case of Intradural Spinal Lipoma
