Balloon Occlusion Retrograde Transvenous Obliteration of Gastric Varices in Two Non-Cirrhotic Patients with Portal Vein Thrombosis
- Affiliations
-
- 1Interventional Radiology, Mallinckrodt Institute of Radiology, Washington University School of Medicine, St. Louis, MO 63110, USA. kims@mir.wustl.edu
- KMID: 1711484
- DOI: http://doi.org/10.3348/kjr.2014.15.1.108
Abstract
- This report describes two non-cirrhotic patients with portal vein thrombosis who underwent successful balloon occlusion retrograde transvenous obliteration (BRTO) of gastric varices with a satisfactory response and no complications. One patient was a 35-year-old female with a history of Crohn's disease, status post-total abdominal colectomy, and portal vein and mesenteric vein thrombosis. The other patient was a 51-year-old female with necrotizing pancreatitis, portal vein thrombosis, and gastric varices. The BRTO procedure was a useful treatment for gastric varices in non-cirrhotic patients with portal vein thrombosis in the presence of a gastrorenal shunt.
Keyword
MeSH Terms
Figure
-
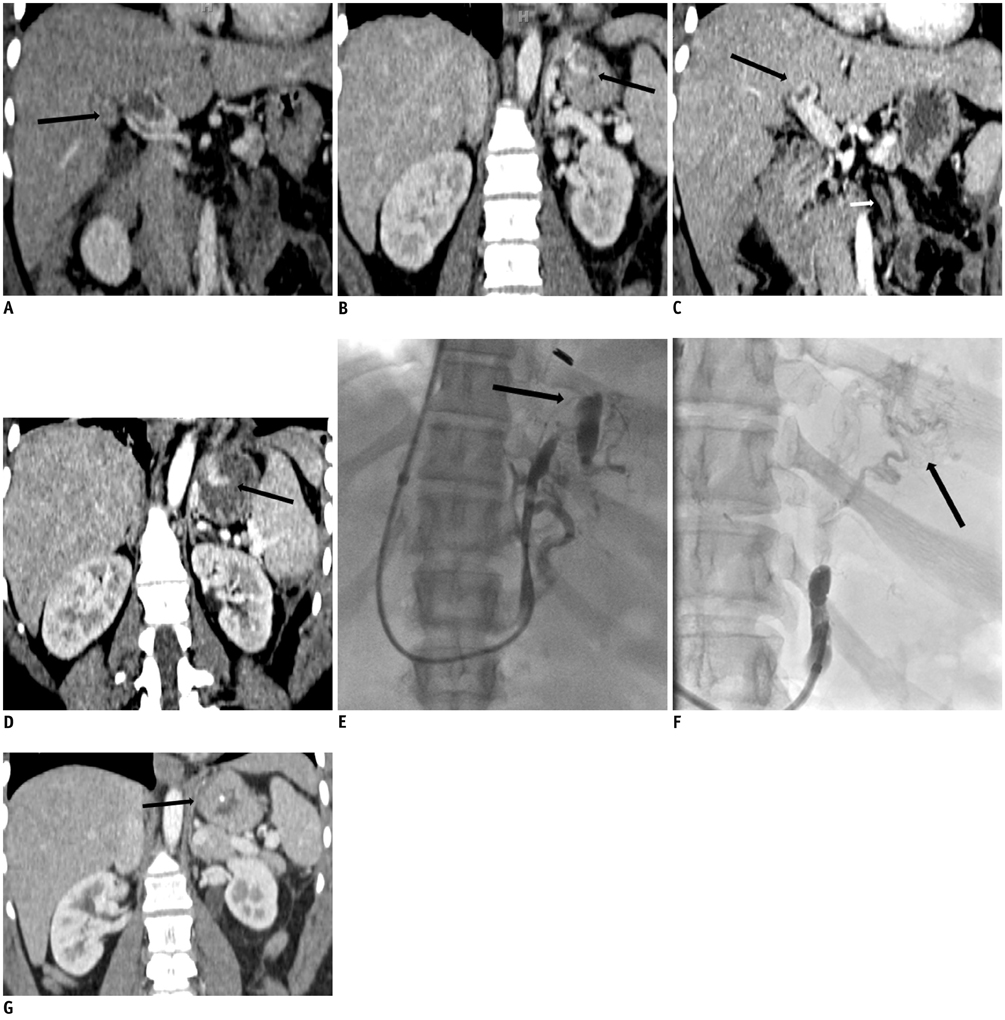
Fig. 1 35-year-old women with history of Crohn's disease, status post total abdominal colectomy, and portal vein and mesenteric vein thrombosis. A, B. Coronal reformatted contrast-enhanced computed tomography (CT) scan 2 weeks after surgery shows large filling defect (arrow) in main portal vein with extension into both right and left portal veins and small isolated varices (arrow) in gastric fundus. C, D. Coronal reformatted contrast-enhanced CT scan at 2 week follow up shows interval decrease in size of portal vein thrombosis, new inferior mesenteric vein thrombosis (small arrow), and interval increase in size of gastric varices (arrow). E. Balloon occluded retrograde venogram shows filling of small gastric varices (arrow). Sclerosant was administered with filling of varices and occlusion balloon inflated. F. Spot image after embolization shows gastric varices with lipiodol uptake (arrow). G. Coronal reformatted contrast-enhanced CT scan 3 months after balloon occlusion retrograde transvenous obliteration procedure shows complete obliteration of gastric fundus with small residual lipiodol uptake (arrow).
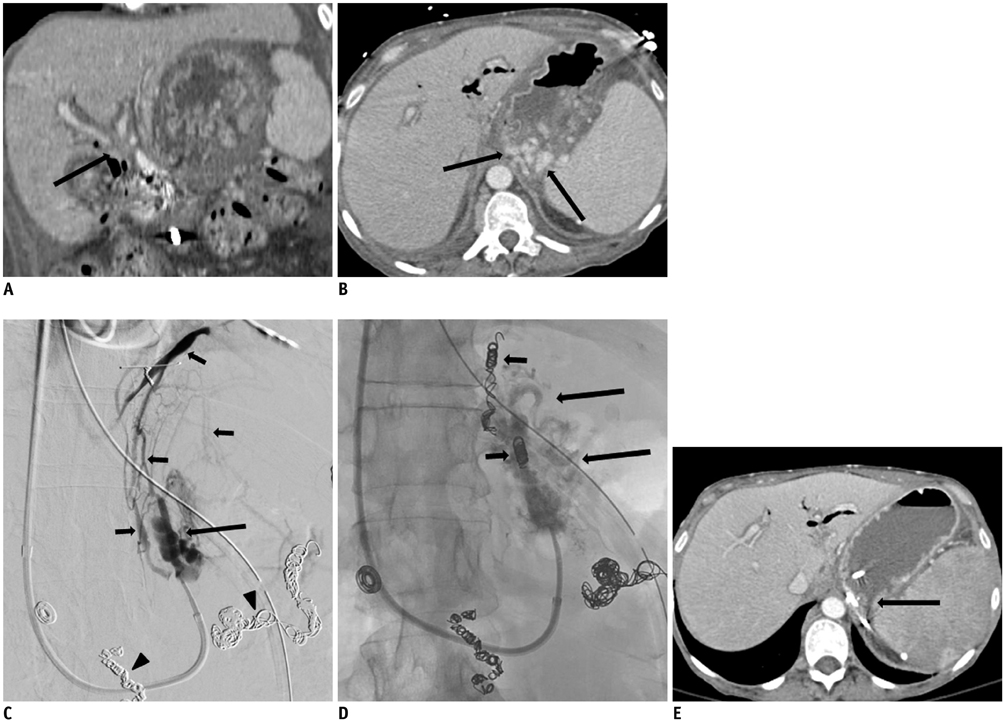
Fig. 2 51-year-old women with necrotizing pancreatitis, portal vein thrombosis, and gastric varices. A, B. Coronal reformatted (A) and axial (B) contrast-enhanced computed tomography (CT) scan 3 days prior to balloon occlusion retrograde transvenous obliteration (BRTO) procedure shows abrupt cut off of both right and left portal veins (arrow), representing portal vein thrombus, splenic vein thrombosis, and enhancing dilated veins (arrows) in region of gastric fundus representing gastric varices. C. Balloon occluded retrograde venogram shows filling of gastric varices (arrow) and multiple collateral veins including inferior phrenic vein (small arrows). Note previous coil embolized splenic and gastroduodenal arteries (arrowheads). Two collateral veins including inferior phrenic vein were embolized with multiple microcoils. Sclerosant was administered with occlusion balloon inflated and filling of varices. D. Spot image of gastric varices post embolization shows gastric varices with lipiodol uptake (arrows) and multiple coils (small arrows) at embolized inferior phrenic vein and small draining vein. E. Axial contrast-enhanced CT scan 6 months after BRTO procedure shows complete obliteration of gastric fundus with small residual lipiodol uptake (arrow).
Reference
-
1. Saad WE, Darcy MD. Transjugular Intrahepatic Portosystemic Shunt (TIPS) versus Balloon-occluded Retrograde Transvenous Obliteration (BRTO) for the Management of Gastric Varices. Semin Intervent Radiol. 2011; 28:339–349.2. Choi YH, Yoon CJ, Park JH, Chung JW, Kwon JW, Choi GM. Balloon-occluded retrograde transvenous obliteration for gastric variceal bleeding: its feasibility compared with transjugular intrahepatic portosystemic shunt. Korean J Radiol. 2003; 4:109–116.3. Thompson RJ, Taylor MA, McKie LD, Diamond T. Sinistral portal hypertension. Ulster Med J. 2006; 75:175–177.4. Kiyosue H, Ibukuro K, Maruno M, Tanoue S, Hongo N, Mori H. Multidetector CT anatomy of drainage routes of gastric varices: a pictorial review. Radiographics. 2013; 33:87–100.5. Remzi FH, Fazio VW, Oncel M, Baker ME, Church JM, Ooi BS, et al. Portal vein thrombi after restorative proctocolectomy. Surgery. 2002; 132:655–661. discussion 661-662.6. Yada S, Hizawa K, Aoyagi K, Hashizume M, Matsumoto T, Koga H, et al. Portal hypertensive gastropathy due to chronic portal vein occlusion in Crohn's disease. Am J Gastroenterol. 1998; 93:1376–1377.7. Gonzelez HJ, Sahay SJ, Samadi B, Davidson BR, Rahman SH. Splanchnic vein thrombosis in severe acute pancreatitis: a 2-year, single-institution experience. HPB (Oxford). 2011; 13:860–864.8. Bockhorn M, Gebauer F, Bogoevski D, Molmenti E, Cataldegirmen G, Vashist YK, et al. Chronic pancreatitis complicated by cavernous transformation of the portal vein: contraindication to surgery? Surgery. 2011; 149:321–328.9. Lin YL, Yang PM, Huang GT, Lee TH, Chau SH, Tsang YM, et al. Variceal bleeding due to segmental portal hypertension caused by chronic pancreatitis. Am J Emerg Med. 1995; 13:676–677.10. Han G, Qi X, He C, Yin Z, Wang J, Xia J, et al. Transjugular intrahepatic portosystemic shunt for portal vein thrombosis with symptomatic portal hypertension in liver cirrhosis. J Hepatol. 2011; 54:78–88.11. Perarnau JM, Baju A, D'alteroche L, Viguier J, Ayoub J. Feasibility and long-term evolution of TIPS in cirrhotic patients with portal thrombosis. Eur J Gastroenterol Hepatol. 2010; 22:1093–1098.12. Bilbao JI, Elorz M, Vivas I, Martínez-Cuesta A, Bastarrika G, Benito A. Transjugular intrahepatic portosystemic shunt (TIPS) in the treatment of venous symptomatic chronic portal thrombosis in non-cirrhotic patients. Cardiovasc Intervent Radiol. 2004; 27:474–480.13. Luo J, Yan Z, Wang J, Liu Q, Qu X. Endovascular treatment for nonacute symptomatic portal venous thrombosis through intrahepatic portosystemic shunt approach. J Vasc Interv Radiol. 2011; 22:61–69.14. Hollingshead M, Burke CT, Mauro MA, Weeks SM, Dixon RG, Jaques PF. Transcatheter thrombolytic therapy for acute mesenteric and portal vein thrombosis. J Vasc Interv Radiol. 2005; 16:651–661.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Balloon-occluded retrograde transvenous obliteration for bleeding gastric varices in a patient without a gastrorenal shunt
- Efficacy and Safety of Balloon-Occluded Retrograde Transvenous Obliteration with Sodium Tetradecyl Sulfate Liquid Sclerotherapy
- Balloon-occluded retrograde transvenous obliteration for six consecutive patients with duodenal varices
- Gastric Varices Treated with Balloon-occluded Retrograde Transvenous Obliteration (BRTO)
- Transjugular intrahepatic portosystemic shunts versus balloon-occluded retrograde transvenous obliteration for the management of gastric varices: Treatment algorithm according to clinical manifestations
