Retrieval Rate and Accuracy of Ultrasound-Guided 14-G Semi-Automated Core Needle Biopsy of Breast Microcalcifications
- Affiliations
-
- 1Department of Radiology, Soonchunhyang University College of Medicine, Bucheon Hospital, Bucheon 420-767, Korea. grace@schmc.ac.kr
- 2Department of Pathology, Soonchunhyang University College of Medicine, Bucheon Hospital, Bucheon 420-767, Korea.
- 3Department of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul 138-736, Korea.
- KMID: 1711472
- DOI: http://doi.org/10.3348/kjr.2014.15.1.12
Abstract
OBJECTIVE
To evaluate the retrieval rate and accuracy of ultrasound (US)-guided 14-G semi-automated core needle biopsy (CNB) for microcalcifications in the breast.
MATERIALS AND METHODS
US-guided 14-G semi-automated CNB procedures and specimen radiography were performed for 33 cases of suspicious microcalcifications apparent on sonography. The accuracy of 14-G semi-automated CNB and radiology-pathology concordance were analyzed and the microcalcification characteristics between groups with successful and failed retrieval were compared.
RESULTS
Thirty lesions were successfully retrieved and the microcalcification retrieval rate was 90.9% (30/33). Thirty lesions were successfully retrieved. Twenty five were finally diagnosed as malignant (10 invasive ductal carcinoma, 15 ductal carcinoma in situ [DCIS]) and five as benign. After surgery and mammographic follow-up, the 25 malignant lesions comprised 12 invasive ductal carcinoma and 13 DCIS. Three lesions in the failed retrieval group (one DCIS and two benign) were finally diagnosed as two DCIS and one benign after surgery. The accuracy of 14-G semi-automated CNB was 90.9% (30/33) because of two DCIS underestimates and one false-negative diagnosis. The discordance rate was significantly higher in the failed retrieval group than in the successful retrieval group (66.7% vs. 6.7%; p < 0.05). Punctate calcifications were significantly more common in the failed retrieval group than in the successful retrieval group (66.7% vs. 3.7%; p < 0.05).
CONCLUSION
US-guided 14-G semi-automated CNB could be a useful procedure for suspicious microcalcifications in the breast those are apparent on sonography.
MeSH Terms
-
Adult
Aged
Biopsy, Large-Core Needle/*methods/standards
Breast/*pathology
Breast Diseases/pathology/radiography
Breast Neoplasms/*pathology/surgery/ultrasonography
Calcinosis/*pathology/ultrasonography
Carcinoma, Ductal, Breast/*pathology/ultrasonography
Carcinoma, Intraductal, Noninfiltrating/*pathology/radiography
Female
Humans
Middle Aged
*Ultrasonography, Interventional/standards
Young Adult
Figure
-
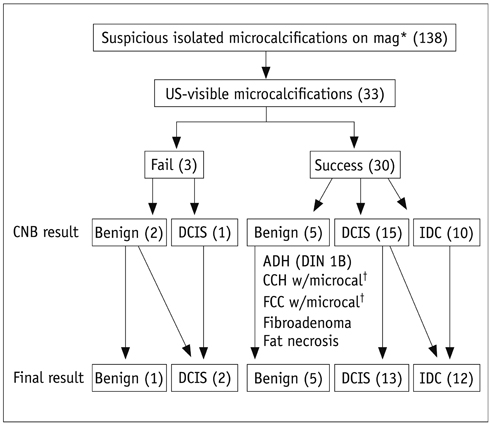
Fig. 1 US-guided 14-G semi-automated core needle biopsy results and pathologic diagnosis of microcalcifications. *Magnification mammography, †Microcalcifications. DCIS = ductal carcinoma in situ, IDC = invasive ductal carcinoma, US = ultrasound, ADH = atypical ductal hyperplasia, DIN = ductal intraepithelial neoplasia, CCH = columnar cell hyperplasia, FCC = fibrocystic changes
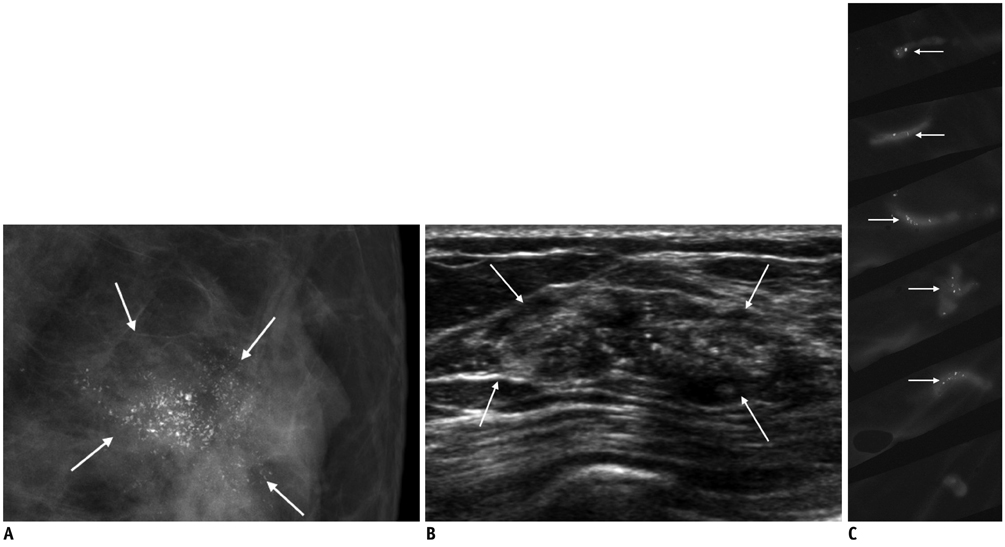
Fig. 2 Details from case of 54-year-old asymptomatic woman. A. Mammography shows clustered fine pleomorphic calcifications (arrows). BI-RADS assessment is category 5. B. Targeted US shows multiple echogenic dots (arrows) within irregular indistinct isoechoic mass. C. Specimen radiography after US-guided 14-G semi-automated CNB shows multiple microcalcifications (arrows) in five of six cores retrieved. Pathology results of both CNB and final surgery were DCIS. BI-RADS = Breast Imaging-Reporting and Data System, US = ultrasound, CNB = core needle biopsy, DCIS = ductal carcinoma in situ
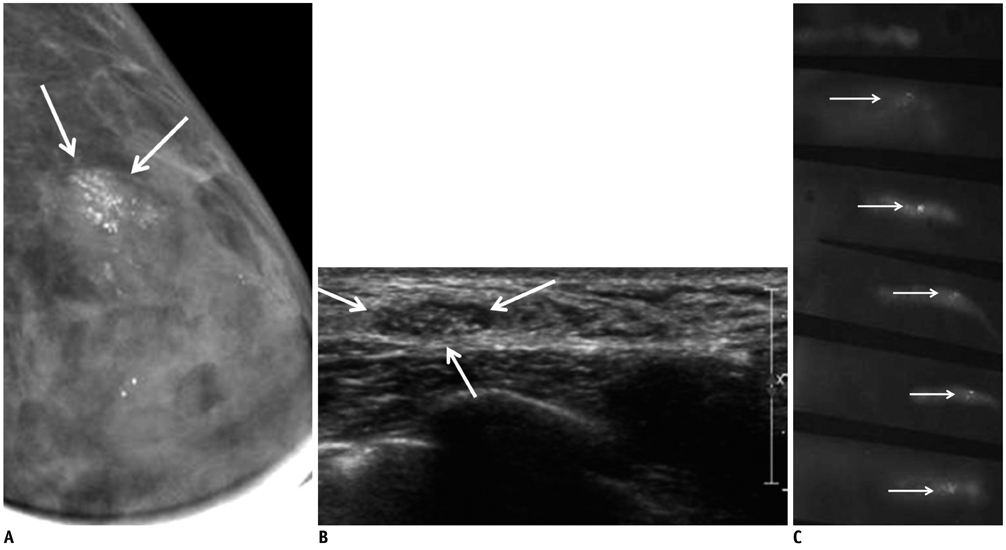
Fig. 3 Details from case of 42-year-old asymptomatic woman. A. Magnification mammography shows compactly clustered fine linear and fine pleomorphic calcifications (arrows). BI-RADS assessment is category 5. B. Targeted US shows multiple microcalcifications (arrows) within oval partially indistinct hypoechoic mass. C. Specimen radiography shows 69 microcalcifications in five (arrows) of six cores retrieved. Pathology result of CNB was columnar cell hyperplasia with microcalcifications and that of mammography-guided localization and surgical excision was fibrocystic change with microcalcifications. BI-RADS = Breast Imaging-Reporting and Data System, US = ultrasound, CNB = core needle biopsy
Cited by 2 articles
-
Annual Trends in Ultrasonography-Guided 14-Gauge Core Needle Biopsy for Breast Lesions
Inha Jung, Kyunghwa Han, Min Jung Kim, Hee Jung Moon, Jung Hyun Yoon, Vivian Youngjean Park, Eun-Kyung Kim
Korean J Radiol. 2020;21(3):259-267. doi: 10.3348/kjr.2019.0695.Clinical Experience of Ultrasound-Guided, Vacuum-Assisted Breast Biopsy for Mammographic Microcalcifications: Combination with Wire Localization
SeungSang Ko, Man Sik Shin, Ki Won Chun, Kang Young Rhee, Heeboong Park
J Surg Ultrasound. 2018;5(2):53-60. doi: 10.46268/jsu.2018.5.2.53.
Reference
-
1. Soo MS, Baker JA, Rosen EL. Sonographic detection and sonographically guided biopsy of breast microcalcifications. AJR Am J Roentgenol. 2003; 180:941–948.2. Liberman L. Percutaneous imaging-guided core breast biopsy: state of the art at the millennium. AJR Am J Roentgenol. 2000; 174:1191–1199.3. Philpotts LE, Hooley RJ, Lee CH. Comparison of automated versus vacuum-assisted biopsy methods for sonographically guided core biopsy of the breast. AJR Am J Roentgenol. 2003; 180:347–351.4. Youk JH, Kim EK, Kim MJ, Lee JY, Oh KK. Missed breast cancers at US-guided core needle biopsy: how to reduce them. Radiographics. 2007; 27:79–94.5. Kim YM, Park HB, Ryu JW. Usefulness of ultrasound-guided mammotome biopsy for microcalcification. J Korean Radiol Soc. 2005; 53:129–135.6. Cho N, Moon WK. Digital mammography-guided skin marking for sonographically guided biopsy of suspicious microcalcifications. AJR Am J Roentgenol. 2009; 192:W132–W136.7. Moon WK, Im JG, Koh YH, Noh DY, Park IA. US of mammographically detected clustered microcalcifications. Radiology. 2000; 217:849–854.8. Teh WL, Wilson AR, Evans AJ, Burrell H, Pinder SE, Ellis IO. Ultrasound guided core biopsy of suspicious mammographic calcifications using high frequency and power Doppler ultrasound. Clin Radiol. 2000; 55:390–394.9. Ciatto S, Houssami N, Ambrogetti D, Bianchi S, Bonardi R, Brancato B, et al. Accuracy and underestimation of malignancy of breast core needle biopsy: the Florence experience of over 4000 consecutive biopsies. Breast Cancer Res Treat. 2007; 101:291–297.10. Kim HS, Kim MJ, Kim EK, Kwak JY, Son EJ, Oh KK. US-guided vacuum-assisted biopsy of microcalcifications in breast lesions and long-term follow-up results. Korean J Radiol. 2008; 9:503–509.11. Cho N, Moon WK, Cha JH, Kim SM, Jang M, Chang JM, et al. Ultrasound-guided vacuum-assisted biopsy of microcalcifications detected at screening mammography. Acta Radiol. 2009; 50:602–609.12. Hahn SY, Shin JH, Han BK, Ko EY. Sonographically-guided vacuum-assisted biopsy with digital mammography-guided skin marking of suspicious breast microcalcifications: comparison of outcomes with stereotactic biopsy in Asian women. Acta Radiol. 2011; 52:29–34.13. American College of Radiology BI-RADS Committee. ACR BIRADS breast imaging and reporting data system: breast imaging atlas. 4th ed. Reston: American College of Radiology;2003.14. Jackman RJ, Burbank F, Parker SH, Evans WP 3rd, Lechner MC, Richardson TR, et al. Stereotactic breast biopsy of nonpalpable lesions: determinants of ductal carcinoma in situ underestimation rates. Radiology. 2001; 218:497–502.15. Hendrick RE, Parker SH. Principle of stereotactic mammography and quality control. In : Parker SH, Jobe WE, editors. Percutaneous Breast Biopsy. New York: Raven;1993. p. 56–58.16. Abdsaleh S, Azavedo E, Lindgren PG. Semiautomatic core biopsy. A modified biopsy technique in breast diseases. Acta Radiol. 2003; 44:47–51.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Usefulness of Ultrasound-Guided Automated Core Biopsy of Nonpalpable Breast Lesions
- Pseudoaneurysm of the Breast after Core Needle Biopsy: A Case Report
- Pseudoaneurysm of the Breast after 14-Gauge Core Biopsy: Case Report
- Breast Lesions with Discordant Results on Ultrasound-guided Core Needle Biopsy
- Clinical Application of Ultrasound-guided Core Needle Biopsy of the Breast
