Correlation of Histological Examination of Meniscus with MR Images: Focused on High Signal Intensity of the Meniscus Not Caused by Definite Meniscal Tear and Impact on MR Diagnosis of Tears
- Affiliations
-
- 1Department of Radiology, Chonbuk National University Hospital, Chonbuk National University College of Medicine, Jeonju 561-712, Korea. sangyleekr@gmail.com
- 2Department of Radiology, Yanbian Second People's Hospital, Yanji, Jilin 133001, China.
- 3Cham Orthopedic Clinic, Jeonju 560-852, Korea.
- 4Department of Orthopedics, Chonbuk National University Hospital, Chonbuk National University College of Medicine, Jeonju 561-712, Korea.
- 5Department of Pathology, Chonbuk National University Hospital, Chonbuk National University College of Medicine, Jeonju 561-712, Korea.
- KMID: 1711461
- DOI: http://doi.org/10.3348/kjr.2013.14.6.935
Abstract
OBJECTIVE
To document the causes of high signal intensity of the meniscus which is not caused by definite meniscal tears on MR imaging, through correlation with histological examination.
MATERIALS AND METHODS
For the correlation between the MR image and histology, we obtained prospectively 31 meniscal specimens from 21 patients. Proton density-weighted turbo spin-echo MR images were used. Minimal tear, thinning of the lamellar layer, degeneration of the central layer, and radial tie fibers were detected upon histological examination, and were correlated with the corresponding MR images.
RESULTS
Minimal tear of the lamellar layer was seen in 60 zones out of 100 slides. On MR images, 29 (48.3%) of these 60 zones had high signal intensity. Thinning of the lamellar layer was seen in 24 zones, with 7 (29.2%) having high signal intensity. 57 central zones showed degenerative change in the central layer and high signal intensity on all corresponding MR images. Radial tie fibers in the central layer appeared as high signal intensity areas.
CONCLUSION
Minimal tear and thinning of the lamellar layer, degeneration and radial tie fibers of the central layer of the meniscus cause high signal intensity on MR images.
Keyword
MeSH Terms
Figure
-
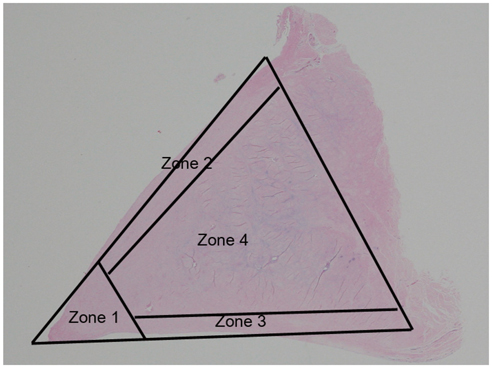
Fig. 1 Meniscal zones. Meniscus is divided into four zones, including apical surface (zone 1), superior lamellar layer (zone 2), inferior lamellar layer (zone 3), and central layer (zone 4). Apical surface (zone 1) is defined as area occupying approximately 20% of inner diameter of meniscus on slide. Superior and inferior lamellar layers are composed of superficial network (about 10 micrometers thick) and lamellar layer (about 150-200 micrometers thick). Four zones of meniscus are drawn on histologic photomicrograph (hematoxylin & eosin staining, 1 : 1) of normal meniscus.
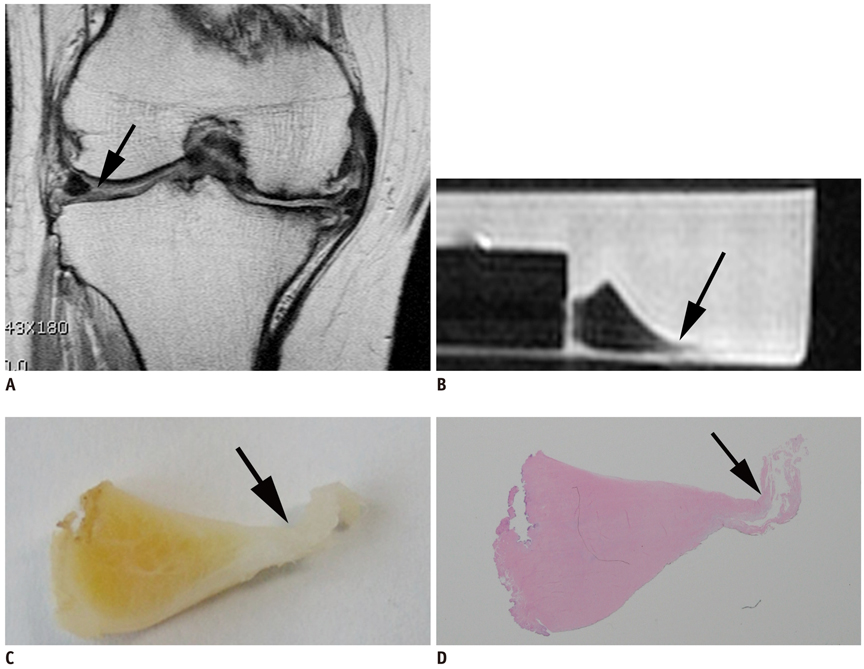
Fig. 2 Fifty-one-year-old female with minimal tear in apical surface, seen as radial tear on preoperative MR image of knee joint. A. Preoperative MR image of body of lateral meniscus shows defect in apical surface (black arrow). B. However, MR image of meniscal specimen obtained from same anatomic section shows abnormally high signal intensity (S1) and surface irregularity (black arrow) (M1). C. Gross meniscal section shows swollen and irregular apical surface of meniscus (black arrow). D. Histologic photomicrograph (hematoxylin & eosin staining, 1 : 1) shows minimal tear of apical surface (black arrow).
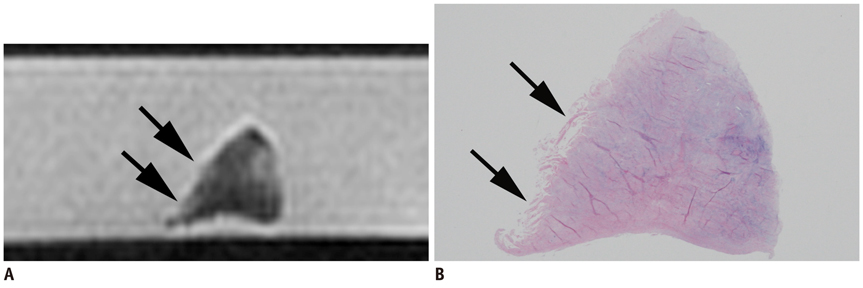
Fig. 3 Seventy-eight-year-old female with minimal tear in superior lamellar layer. A. MR image of meniscal section shows high signal intensity (S1) and surface irregularity (M1) (black arrows) in superior lamellar layer. B. Histologic photomicrograph (hematoxylin & eosin staining, 1 : 1) shows minimal tear in superior lamellar layer and apical surface (black arrows).
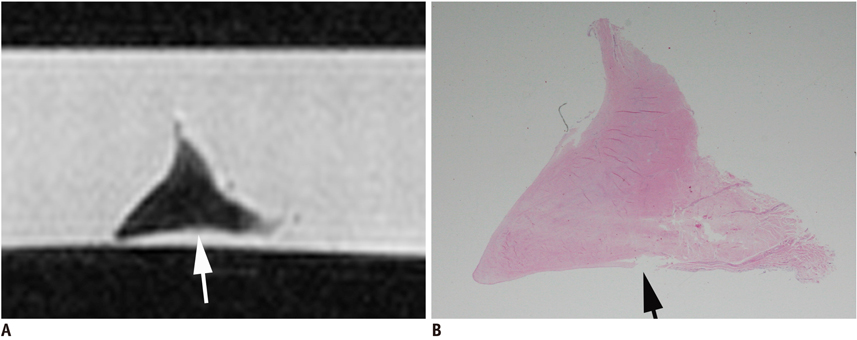
Fig. 4 Seventy-eight-year-old male with meniscal thinning. A. MR imaging of medial meniscus shows surface irregularity on inferior lamellar layer (white arrow). B. Photomicrograph (hematoxylin & eosin staining, 1 : 1) shows thinning of inferior lamellar layer (black arrow).
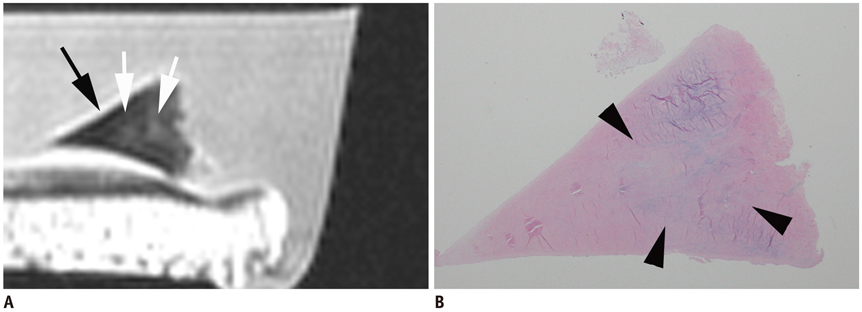
Fig. 5 Sixty-eight-year-old female with degeneration of central layer. A. MR image of meniscus shows abnormal high signal intensity (S1) in central layer (white arrows), but both superior and inferior lamellar layers show normal dark signal intensities (black arrow). B. Histologic photomicrograph (hematoxylin & eosin staining, 1 : 1) shows degenerative changes in central layer (arrowheads), but exact one-to-one correlation between abnormal high signal intensity of MR image and detection of degenerative changes on histologic slide was not possible because boundary of degeneration could not clearly be determined on histologic slide.

Fig. 6 Sixty-eight-year-old female with MR Grade 3 signal intensity (A, B), and 60-year-old female with minimal tear of superior lamellar layer, which is distant from degeneration of central layer (C, D). A. On histologic photomicrograph (hematoxylin & eosin staining, 1 : 1), minimal tear of superior lamellar layer (black arrow) is connected to degeneration of central layer (asterisk). B. MR image of same section shows MR grade 3 signal intensity (black arrow), in which abnormally high signal intensity of minimal tear is connected to high signal intensity of adjacent central layer of meniscus (asterisk). C, D. MR image shows high signal intensity and surface irregularity due to minimal tear (black arrows) of superior lamellar layer, which is confirmed on histologic slide D (hematoxylin & eosin staining, 1 : 1). Ovoid-shaped high signal intensity of central layer on MR image (asterisk in C), which is distant from minimal tear of superior lamellar layer, is shown to be degeneration of central layer on histological examination (asterisks in D). MR finding of this meniscal specimen was considered to be of grade 2 signal intensity.
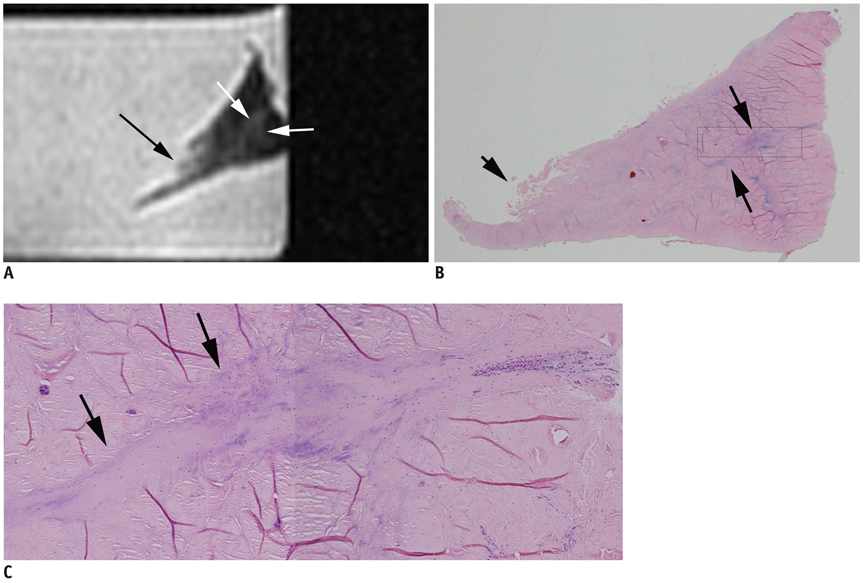
Fig. 7 Eighty-two-year-old female with radial tie fibers. A. High signal intensity in linear pattern (white arrows) is demonstrated in central layer of meniscus. B. Radial tie fibers in linear pattern (long black arrows) are seen on histologic slide (hematoxylin & eosin staining, 1 : 1). C. Rectangle from B. Detailed histologic photomicrograph (C, hematoxyolin & eosin staining, × 10) shows loose connective tissue (radial tie fibers) (black arrows) penetrating radially from joint capsule between circular fibrils of central layer. Minimal tear of apical surface is seen on MR image (long black arrow in A) and histologic photographs (short black arrow in B).
Reference
-
1. Grossman JW, De Smet AA, Shinki K. Comparison of the accuracy rates of 3-T and 1.5-T MRI of the knee in the diagnosis of meniscal tear. AJR Am J Roentgenol. 2009; 193:509–514.2. Quinn SF, Brown TF. Meniscal tears diagnosed with MR imaging versus arthroscopy: how reliable a standard is arthroscopy? Radiology. 1991; 181:843–847.3. De Smet AA, Tuite MJ, Norris MA, Swan JS. MR diagnosis of meniscal tears: analysis of causes of errors. AJR Am J Roentgenol. 1994; 163:1419–1423.4. Justice WW, Quinn SF. Error patterns in the MR imaging evaluation of menisci of the knee. Radiology. 1995; 196:617–621.5. Lotysch M, Mink J, Crues JV, Schwartz SA. Magnetic resonance imaging in the detection of meniscal injuries (abstract). Magn Reson Imaging. 1986; 4:185.6. Negendank WG, Fernandez-Madrid FR, Heilbrun LK, Teitge RA. Magnetic resonance imaging of meniscal degeneration in asymptomatic knees. J Orthop Res. 1990; 8:311–320.7. Dillon EH, Pope CF, Jokl P, Lynch K. The clinical significance of stage 2 meniscal abnormalities on magnetic resonance knee images. Magn Reson Imaging. 1990; 8:411–415.8. McCauley TR, Jee WH, Galloway MT, Lynch K, Jokl P. Grade 2C signal in the meniscus [correction of mensicus] on MR imaging of the knee. AJR Am J Roentgenol. 2002; 179:645–648.9. De Smet AA, Tuite MJ. Use of the "two-slice-touch" rule for the MRI diagnosis of meniscal tears. AJR Am J Roentgenol. 2006; 187:911–914.10. Escobedo EM, Hunter JC, Zink-Brody GC, Wilson AJ, Harrison SD, Fisher DJ. Usefulness of turbo spin-echo MR imaging in the evaluation of meniscal tears: comparison with a conventional spin-echo sequence. AJR Am J Roentgenol. 1996; 167:1223–1227.11. Petersen W, Tillmann B. Collagenous fibril texture of the human knee joint menisci. Anat Embryol (Berl). 1998; 197:317–324.12. Stoller DW, Martin C, Crues JV 3rd, Kaplan L, Mink JH. Meniscal tears: pathologic correlation with MR imaging. Radiology. 1987; 163:731–735.13. Araki Y, Ootani F, Tsukaguchi I, Ootani M, Furukawa T, Yamamoto T, et al. MR diagnosis of meniscal tears of the knee: value of axial three-dimensional Fourier transformation GRASS images. AJR Am J Roentgenol. 1992; 158:587–590.14. Disler DG, Kattapuram SV, Chew FS, Rosenthal DI, Patel D. Meniscal tears of the knee: preliminary comparison of three-dimensional MR reconstruction with two-dimensional MR imaging and arthroscopy. AJR Am J Roentgenol. 1993; 160:343–345.15. Quinn SF, Brown TR, Szumowski J. Menisci of the knee: radial MR imaging correlated with arthroscopy in 259 patients. Radiology. 1992; 185:577–580.16. Smith DK, Totty WG. The knee after partial meniscectomy: MR imaging features. Radiology. 1990; 176:141–144.17. Deutsch AL, Mink JH, Fox JM, Friedman MJ, Howell SM. The postoperative knee. Magn Reson Q. 1992; 8:23–54.18. Deutsch AL, Mink JH, Fox JM, Arnoczky SP, Rothman BJ, Stoller DW, et al. Peripheral meniscal tears: MR findings after conservative treatment or arthroscopic repair. Radiology. 1990; 176:485–488.19. Farley TE, Howell SM, Love KF, Wolfe RD, Neumann CH. Meniscal tears: MR and arthrographic findings after arthroscopic repair. Radiology. 1991; 180:517–522.20. Van Dyck P, Gielen J, D'Anvers J, Vanhoenacker F, Dossche L, Van Gestel J, et al. MR diagnosis of meniscal tears of the knee: analysis of error patterns. Arch Orthop Trauma Surg. 2007; 127:849–854.21. Noble J, Hamblen DL. The pathology of the degenerate meniscus lesion. J Bone Joint Surg Br. 1975; 57:180–186.22. Hodler J, Haghighi P, Pathria MN, Trudell D, Resnick D. Meniscal changes in the elderly: correlation of MR imaging and histologic findings. Radiology. 1992; 184:221–225.23. Skaggs DL, Warden WH, Mow VC. Radial tie fibers influence the tensile properties of the bovine medial meniscus. J Orthop Res. 1994; 12:176–185.24. Hauger O, Frank LR, Boutin RD, Lektrakul N, Chung CB, Haghighi P, et al. Characterization of the "red zone" of knee meniscus: MR imaging and histologic correlation. Radiology. 2000; 217:193–200.25. Bullough PG, Munuera L, Murphy J, Weinstein AM. The strength of the menisci of the knee as it relates to their fine structure. J Bone Joint Surg Br. 1970; 52:564–567.26. Cameron HU, Macnab I. The structure of the meniscus of the human knee joint. Clin Orthop Relat Res. 1972; 89:215–219.27. Ferrer-Roca O, Vilalta C. Lesions of the meniscus. Part I: Macroscopic and histologic findings. Clin Orthop Relat Res. 1980; 289–300.28. Mow VC, Ratcliffe A, Chem KY, Kelly MA. Structure and function relationship of the meniscus of the knee. In : Mow VC, Aronoczky SP, Jackson DW, editors. Knee meniscus: basis and clinical foundations. New York: Raven Press;1992. p. 45–47.29. Takeda Y, Ikata T, Yoshida S, Takai H, Kashiwaguchi S. MRI high-signal intensity in the menisci of asymptomatic children. J Bone Joint Surg Br. 1998; 80:463–467.30. Kornick J, Trefelner E, McCarthy S, Lange R, Lynch K, Jokl P. Meniscal abnormalities in the asymptomatic population at MR imaging. Radiology. 1990; 177:463–465.
