Congenital Variants and Anomalies of the Pancreas and Pancreatic Duct: Imaging by Magnetic Resonance Cholangiopancreaticography and Multidetector Computed Tomography
- Affiliations
-
- 1Department of Radiology, Turkiye Yuksek Ihtisas Hospital, Kizilay street, No:4, 06100, Sihhiye, Ankara, Turkey. aturkvatan@yahoo.com
- 2Department of Radiology, Ankara University School of Medicine, Talatpasa Street, 06100, Sihhiye, Ankara, Turkey.
- 3Department of General Surgery, Antalya University School of Medicine, Dumlupinar Street, 07058, Antalya, Turkey.
- KMID: 1711456
- DOI: http://doi.org/10.3348/kjr.2013.14.6.905
Abstract
- Though congenital anomalies of the pancreas and pancreatic duct are relatively uncommon and they are often discovered as an incidental finding in asymptomatic patients, some of these anomalies may lead to various clinical symptoms such as recurrent abdominal pain, nausea and vomiting. Recognition of these anomalies is important because these anomalies may be a surgically correctable cause of recurrent pancreatitis or the cause of gastric outlet obstruction. An awareness of these anomalies may help in surgical planning and prevent inadvertent ductal injury. The purpose of this article is to review normal pancreatic embryology, the appearance of ductal anatomic variants and developmental anomalies of the pancreas, with emphasis on magnetic resonance cholangiopancreaticography and multidetector computed tomography.
MeSH Terms
Figure
-
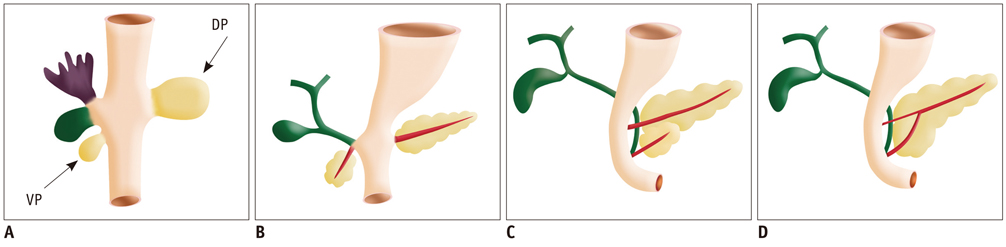
Fig. 1 Drawings show normal embrologic development of pancreas. Ventral pancreatic bud (VP) arises from hepatic diverticulum, and dorsal pancreatic bud (DP) arises from dorsal mesogastrium (A). During 7th gestational week, expansion of duodenum causes ventral pancreatic bud to rotate and pass behind duodenum from right to left and fuse with dorsal pancreatic bud (B-D). Ventral bud forms posterior head and uncinate process, whereas dorsal bud forms anterior head, body, and tail. Finally, ventral and dorsal pancreatic ducts fuse, and pancreas predominantly is drained through ventral duct, which joins common bile duct at level of major papilla and dorsal duct drains at level of minor papilla.
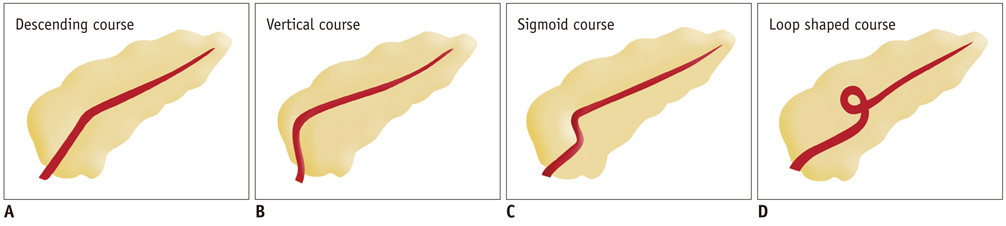
Fig. 2 Drawings show variation in course of pancreatic duct. (A) Descending (B) vertical (C) sigmoid (D) loop shaped course.
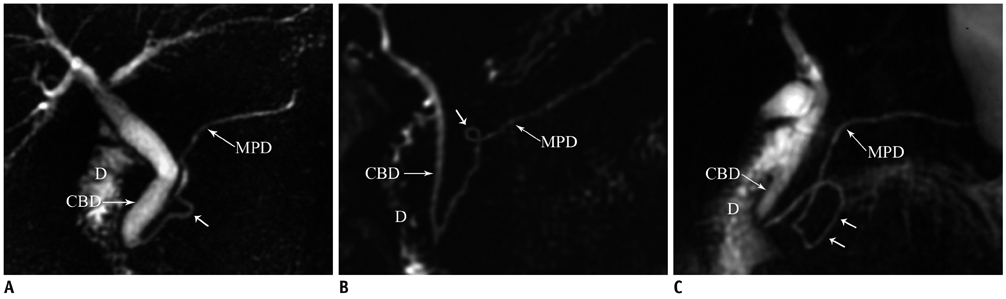
Fig. 3 Magnetic resonance cholangiopancreaticography images reveal variation in course of pancreatic duct. A. Sigmoid shaped (arrow). B, C. loop shaped (arrows) course. CBD = common bile duct, D = duodenum, MPD = main pancreatic duct
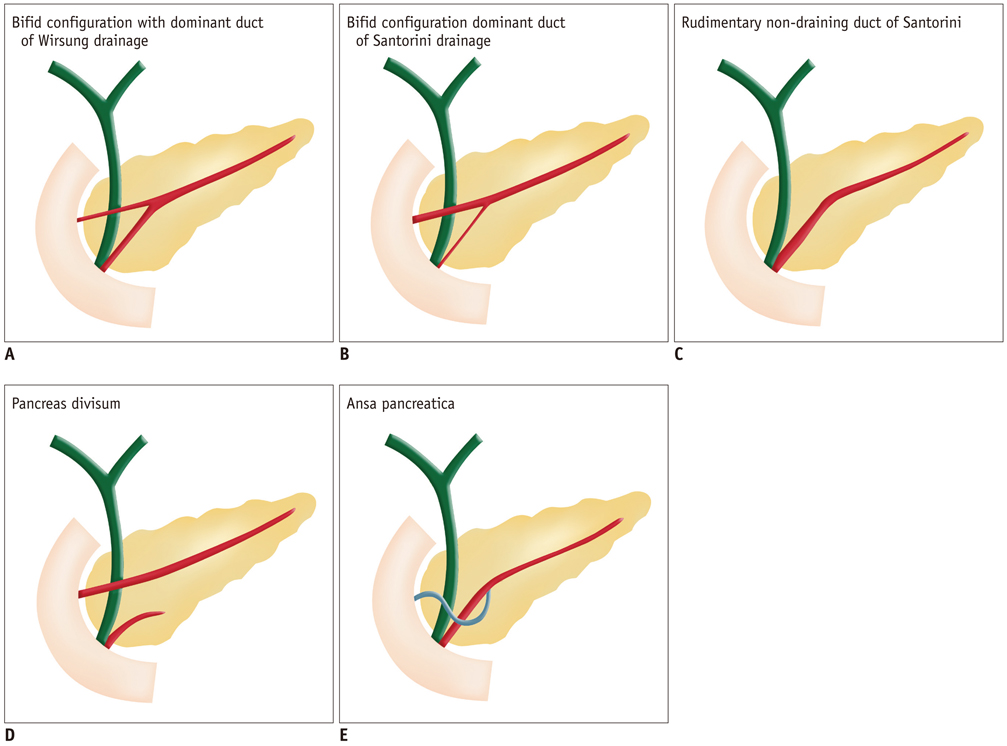
Fig. 4 Drawings show variation in configuration of pancreatic duct. (A) Bifid configuration with dominant duct of Wirsung drainage, (B) bifid configuration with dominant duct of Santorini drainage without divisum, (C) rudimentary non-draining duct of Santorini (D) pancreas divisum, (E) ansa pancreatica.
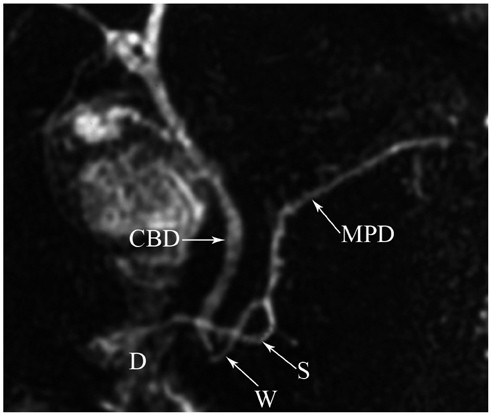
Fig. 5 Magnetic resonance cholangiopancreaticography image reveals typical inverted-S shape of duct of Santorini (S) in ansa pancreatica. CBD = common bile duct, D = duodenum, MPD = main pancreatic duct, W = Wirsung
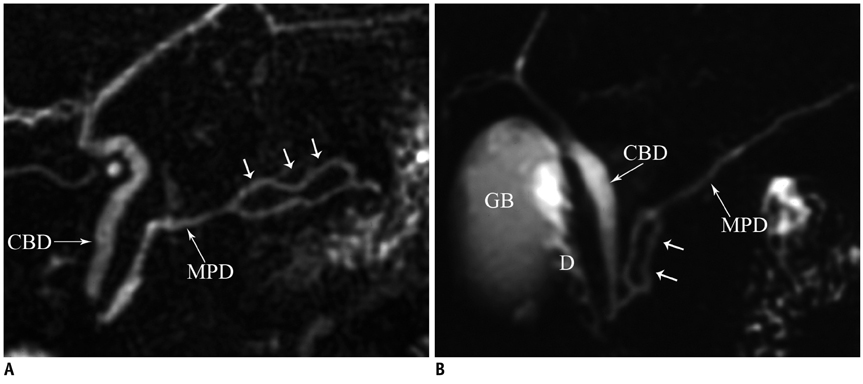
Fig. 6 Duplication of pancreatic duct. Magnetic resonance cholangiopancreaticography images (A, B) show focal duplication (arrows) of pancreatic duct. CBD = common bile duct, D = duodenum, GB = gall bladder, MPD = main pancreatic duct
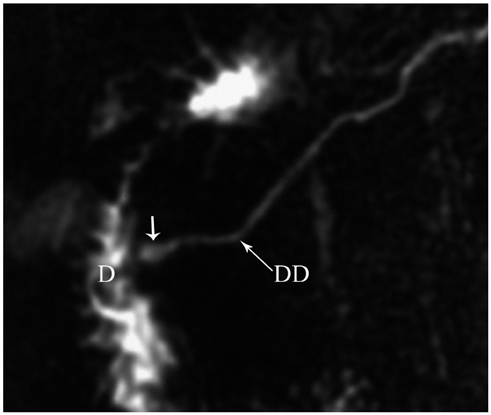
Fig. 7 Magnetic resonance cholangiopancreaticography image reveals dominant dorsal duct (DD) with santorinicele (arrow) in pancreas divisum. D = duodenum
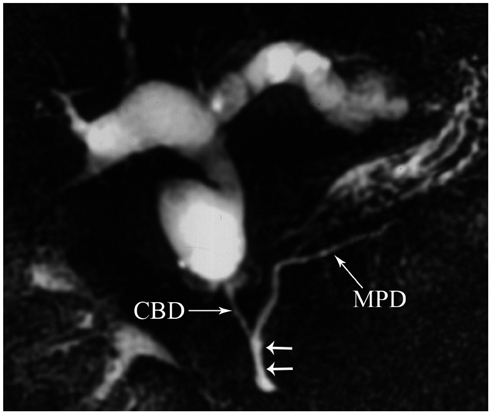
Fig. 8 Magnetic resonance cholangiopancreaticography image reveals long common channel (> 15 mm) (arrows) and associated Todani type 4a choledochal cysts with intrahepatic and extrahepatic components. CBD = common bile duct, MPD = main pancreatic duct
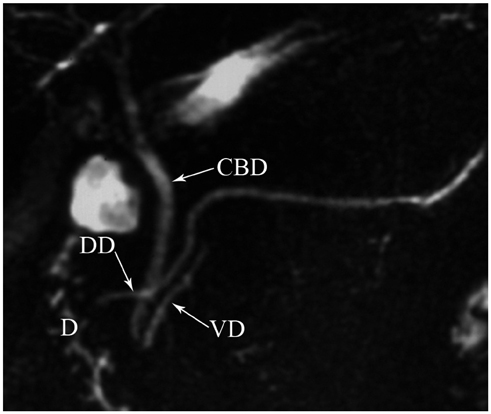
Fig. 9 Magnetic resonance cholangiopancreaticography image shows dorsal duct (DD) crossing anterior to common bile duct (CBD) and emptying separately into minor papilla and CBD joining with ventral duct (VD) and both entering into major papilla in patient with pancreas divisum. D = duodenum
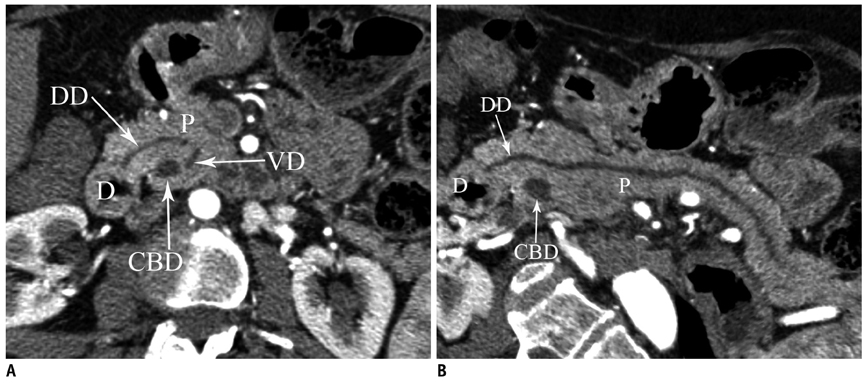
Fig. 10 Pancreas divisum. Axial (A) and curved planar reformatted (B) MDCT images show dorsal duct (DD) crossing anterior to common bile duct (CBD) and emptying separately into minor papilla in patient with pancreas divisum. D = duodenum, P = pancreas, VD = ventral duct, MDCT = multidetector computed tomography
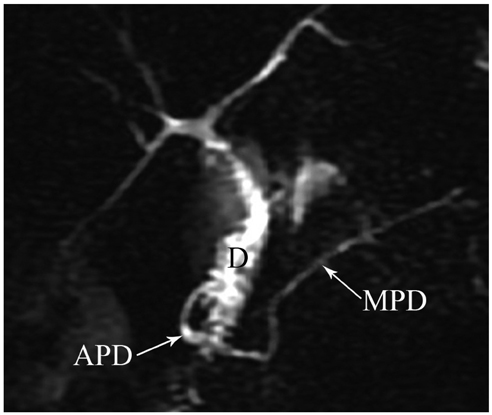
Fig. 11 Magnetic resonance cholangiopancreaticography image shows annular pancreatic duct (APD) communicating with main pancreatic duct (MPD) and completely encircling duodenum (D) in patient with annular pancreas.
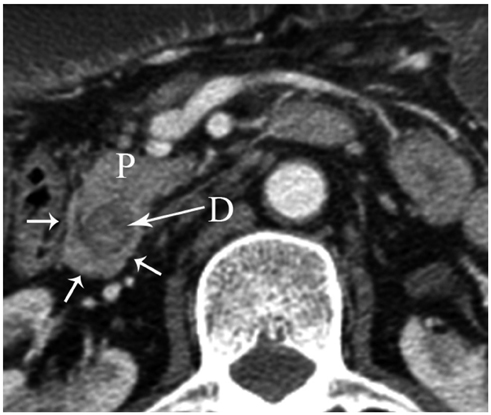
Fig. 12 Axial MDCT image shows pancreatic tissue (arrows) completely encircling second part of duodenum (D) in patient with annular pancreas. P = pancreas, MDCT = multidetector computed tomography
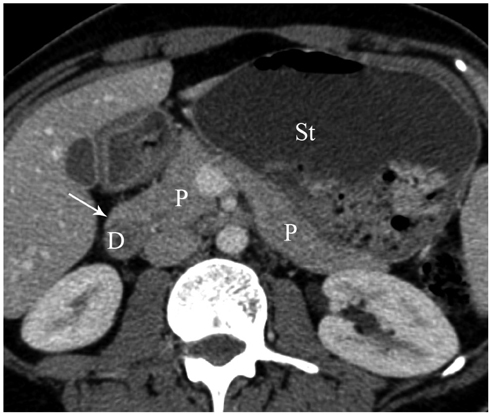
Fig. 13 Axial MDCT image shows pancreatic tissue (arrow) extending in anterolateral direction to second part of duodenum (D) and dilatation of stomach (St) in patient with incomplete annular pancreas. P = pancreas, MDCT = multidetector computed tomography

Fig. 14 Axial MDCT image shows partial dorsal agenesis of pancreas (arrows) in patient with polysplenia syndrome. P = pancreas, J = jejunum, S = spleen, MDCT = multidetector computed tomography
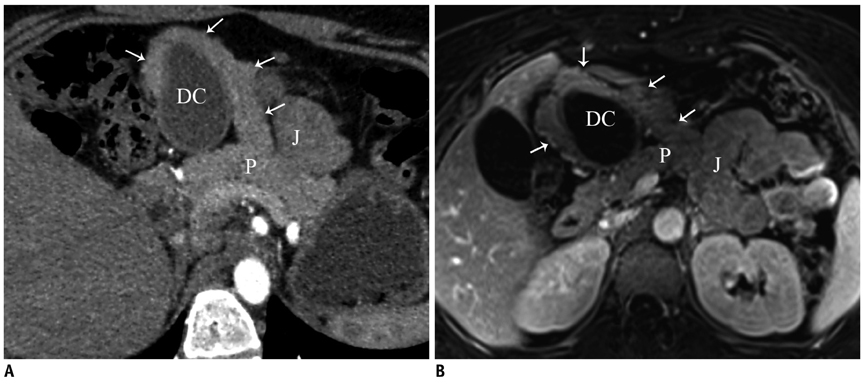
Fig. 15 Accessory pancreatic lobe. Oblique axial (A) and fat suppressed contrast-enhanced T1-weighted gradient echo (B) MR images show accessory pancreatic lobe (arrows) that has similar attenuation and signal intensity to pancreatic tissue (P), arising from pancreas, projecting anteriorly and attaching to gastric duplication cyst (DC). P = pancreas, J = jejunum
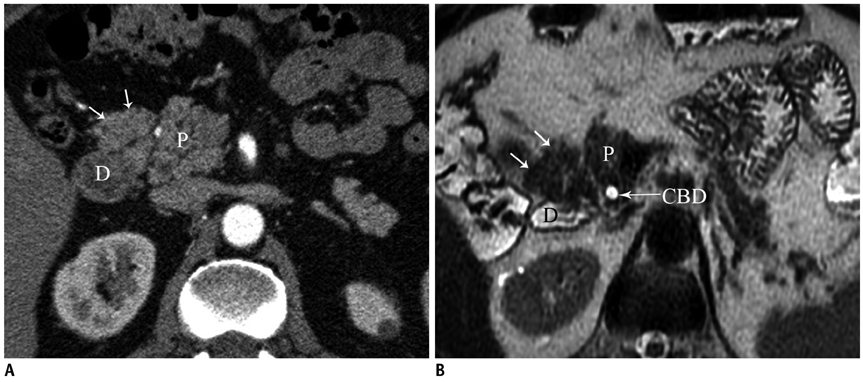
Fig. 16 Variations of pancreatic contours. Axial MDCT (A) and T2-weighted MR (B) images show soft tissue protuberance (arrows) that has similar attenuation and signal intensity to pancreatic head (P). C = common bile duct, CBD = common biliary duct, D = duodenum, P = pancreas
Cited by 2 articles
-
A rare case of choledochal cyst with pancreas divisum: case presentation and literature review
Adrián Ransom-Rodríguez, Ruben Blachman-Braun, Emilio Sánchez-García Ramos, Jesús Varela-Prieto, Erick Rosas-Lezama, Miguel Ángel Mercado
Ann Hepatobiliary Pancreat Surg. 2017;21(1):52-56. doi: 10.14701/ahbps.2017.21.1.52.Exploring the variations of the pancreatic ductal system: a systematic review and meta-analysis of observational studies
Adil Asghar, Ravi Kant Narayan, Nagavalli Basavanna Pushpa, Apurba Patra, Kumar Satish Ravi, R. Shane Tubbs
Anat Cell Biol. 2024;57(1):31-44. doi: 10.5115/acb.23.148.
Reference
-
1. Itoh S, Ikeda M, Ota T, Satake H, Takai K, Ishigaki T. Assessment of the pancreatic and intrapancreatic bile ducts using 0.5-mm collimation and multiplanar reformatted images in multislice CT. Eur Radiol. 2003; 13:277–285.2. Itoh S, Fukushima H, Takada A, Suzuki K, Satake H, Ishigaki T. Assessment of anomalous pancreaticobiliary ductal junction with high-resolution multiplanar reformatted images in MDCT. AJR Am J Roentgenol. 2006; 187:668–675.3. Schulte SJ. Embryology, normal variation, and congenital anomalies of the pancreas. In : Stevenson GW, Freeny PC, Margulis AR, Burhenne HJ, editors. Margulis' and Burhenne's alimentary tract radiology. 5th ed. St. Louis: Mosby;1994. p. 1039–1051.4. Mortelé KJ, Rocha TC, Streeter JL, Taylor AJ. Multimodality imaging of pancreatic and biliary congenital anomalies. Radiographics. 2006; 26:715–731.5. Cha SW, Park MS, Kim KW, Byun JH, Yu JS, Kim MJ, et al. Choledochal cyst and anomalous pancreaticobiliary ductal union in adults: radiological spectrum and complications. J Comput Assist Tomogr. 2008; 32:17–22.6. Kozu T, Suda K, Toki F. Pancreatic development and anatomical variation. Gastrointest Endosc Clin N Am. 1995; 5:1–30.7. Quest L, Lombard M. Pancreas divisum: opinio divisa. Gut. 2000; 47:317–319.8. Soto JA, Lucey BC, Stuhlfaut JW. Pancreas divisum: depiction with multi-detector row CT. Radiology. 2005; 235:503–508.9. Sandrasegaran K, Patel A, Fogel EL, Zyromski NJ, Pitt HA. Annular pancreas in adults. AJR Am J Roentgenol. 2009; 193:455–460.10. Rizzo RJ, Szucs RA, Turner MA. Congenital abnormalities of the pancreas and biliary tree in adults. Radiographics. 1995; 15:49–68. quiz 147-148.11. Nijs EL, Callahan MJ. Congenital and developmental pancreatic anomalies: ultrasound, computed tomography, and magnetic resonance imaging features. Semin Ultrasound CT MR. 2007; 28:395–401.12. Yu J, Turner MA, Fulcher AS, Halvorsen RA. Congenital anomalies and normal variants of the pancreaticobiliary tract and the pancreas in adults: part 2, Pancreatic duct and pancreas. AJR Am J Roentgenol. 2006; 187:1544–1553.13. Emerson L, Layfield LJ, Rohr LR, Dayton MT. Adenocarcinoma arising in association with gastric heterotopic pancreas: a case report and review of the literature. J Surg Oncol. 2004; 87:53–57.14. Alexander LF. Congenital pancreatic anomalies, variants, and conditions. Radiol Clin North Am. 2012; 50:487–498.15. Low JP, Williams D, Chaganti JR. Polysplenia syndrome with agenesis of the dorsal pancreas and preduodenal portal vein presenting with obstructive jaundice--a case report and literature review. Br J Radiol. 2011; 84:e217–e220.16. Lång K, Lasson A, Müller MF, Thorlacius H, Toth E, Olsson R. Dorsal agenesis of the pancreas - a rare cause of abdominal pain and insulin-dependent diabetes. Acta Radiol. 2012; 53:2–4.17. Oeda S, Otsuka T, Akiyama T, Ario K, Masuda M, Taguchi S, et al. Recurrent acute pancreatitis caused by a gastric duplication cyst communicating with an aberrant pancreatic duct. Intern Med. 2010; 49:1371–1375.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pancreas Neuroendocrine Tumor and Its Mimics: Review of Cross-Sectional Imaging Findings for Differential Diagnosis
- Preoperative Radiologic Evaluation of Cholangiocarcinoma
- Imaging Findings of Primary Angiomyolipoma of the Pancreas: A Case Report
- Squamous Cell Carcinoma of the Pancreas: A Case Report
- Aortic Arch Variants and Anomalies: Embryology, Imaging Findings, and Clinical Considerations
