Korean J Clin Neurophysiol.
2014 Jun;16(1):27-31. 10.14253/kjcn.2014.16.1.27.
A Case of Wernicke's Encephalopathy Presenting as Acute Bilateral Wrist Drop
- Affiliations
-
- 1Department of Neurology, Chonbuk National University College of Medicine, Jeonju, Korea. ohsun@jbnu.ac.kr
- 2Biomedical Research Institute of Chonbuk National University Hospital, Jeonju, Korea.
- KMID: 1708888
- DOI: http://doi.org/10.14253/kjcn.2014.16.1.27
Abstract
- Thiamine deficiency can cause peripheral polyneuropathy and Wernicke's encephalopathy. Wernicke's encephalopathy is characterized by ataxia, ophthalmoplegia, nystagmus, and confusion, and typically presents acute and rapidly progressive course, whereas peripheral neuropathy associated with thiamine deficiency manifests chronic and slowly progressive one. However, acute and rapidly progressive axonal polyneuropathy combined with Wernicke's encephalopathy is quite rare and unusual. Here, we describe a patient with Wernicke's encephalopathy who presented with acute bilateral axonal neuropathy.
MeSH Terms
Figure
-
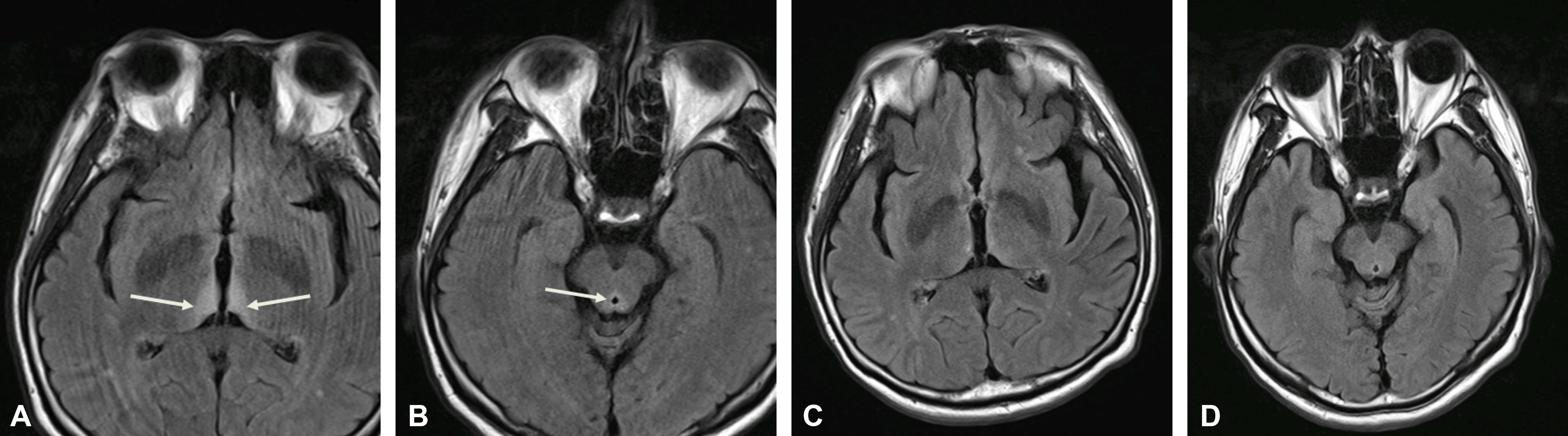
Figure 1. Coronal fluid attenuated inversion recovery (FLAIR) MR images. These FLAIR images show signal intensity alterations of medial thalamus (white arrows, A) and periaqueductal area of the midbrain (white arrow, B) in an acute period of disease. After six weeks of treatment, follow-up FLAIR MR images (C and D) showed a normalized signal change in same area (A and B level) that affected by Wernicke's encephalopathy.
Reference
-
1.Thomson AD., Guerrini I., Marshall EJ. Wernicke's encephalopathy: role of thiamine. Practical Gastroenterol. 2009. 75:21–30.2.Donnino MW., Vega J., Miller J., Walsh M. Myths and misconceptions of Wernicke's encephalopathy: what every emergency physician should know. Ann Emerg Med. 2007. 50:715–721.
Article3.Butterworth RF. Thiamin deficiency and brain disorders. Nutr. Res. Rev. 2003. 16:277–283.
Article4.Lehmann HC., Lindenberg R., Arendt G., Ploner M. Acute axonal neuropathy and Wernicke's encephalopathy. J Neurol. 2006. 253:1516–1517.
Article5.Koike H., Misu K., Hattori N., Ito S., Ichimura M., Ito H, et al. Postgastrectomy polyneuropathy with thiamine deficiency. J Neurol Neurosurg Psychiatry. 2001. 71:357–362.
Article6.Zuccoli G., Pipitone N. Neuroimaging findings in acute Wernicke's encephalopathy: review of the literature. AJR Am J Roentgenol. 2009. 192:501–508.
Article7.Ishibashi S., Yokota T., Shiojiri T., Matunaga T., Tanaka H., Nishina K, et al. Reversible acute axonal polyneuropathy associated with Wernicke-Korsakoff syndrome: impaired physiological nerve conduction due to thiamine deficiency? J Neurol Neurosurg Psychiatry. 2003. 74:674–676.
Article8.Thaisetthawatkul P., Collazo-Clavell ML., Sarr MG., Norell JE., Dyck PJ. A controlled study of peripheral neuropathy after bariatric surgery. Neurology. 2004. 63:1462–1470.
Article9.Galvin R., Bråthen G., Ivashynka A., Hillbom M., Tanasescu R., Leone MA. EFNS guidelines for diagnosis, therapy and prevention of Wernicke encephalopathy. Eur J Neurol. 2010. 17:1408–1418.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Wernicke's Encephalopathy with Hyperemesis Gravidarum
- Wernicke Encephalopathy Associated with Acute Wet Beriberi
- Bilateral Hearing Loss in Wernicke Encephalopathy
- A Case of Wernicke's Encephalopathy Associated with Hyperemesis Gravidarum
- Wernicke's Encephalopathy Presenting with Bilateral Complete Horizontal and Downward Gaze Palsy in a Malnourished Patient
