Thyroid Ultrasonography: Pitfalls and Techniques
- Affiliations
-
- 1Department of Radiology, Research Institute of Radiological Science, Yonsei University College of Medicine, Seoul 120-752, Korea. docjin@yuhs.ac
- 2Department of Radiology, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul 110-746, Korea.
- 3Department of Radiology, Chung-Ang University Hospital, Seoul 156-755, Korea.
- KMID: 1705583
- DOI: http://doi.org/10.3348/kjr.2014.15.2.267
Abstract
- Thyroid ultrasonography (US) plays a key role in the diagnosis and management of thyroid-related diseases. The aim of this article was to illustrate various pitfalls that can occur in utilizing thyroid US and techniques to prevent them. In this article, we present cases demonstrating the common pitfalls associated with US equipment, performance, normal thyroid structures, misinterpretations, and surrounding structures. Knowledge of these areas is essential to avoid misdiagnosis or improper disease management.
Keyword
MeSH Terms
Figure
-

Fig. 1 Normal transverse US of thyroid gland. Cross-sectional US shows normal thyroid glands and surrounding structures. Both thyroid glands show homogeneous parenchymal echogenicity higher than anterior strap muscles. Both CCAs run laterally adjacent to both thyroid lobes and infrahyoid strap muscles overlie thyroid gland. Both SCM muscles are located antero-laterally and longus colli muscles are seen posterolaterally to thyroid gland. US = ultrasonography, SCM = sternocleidomastoid muscle, CCA = common carotid artery, IJV = internal jugular vein, Ant. Strap m = anterior strap muscle, Longus Colli m = longus colli muscle
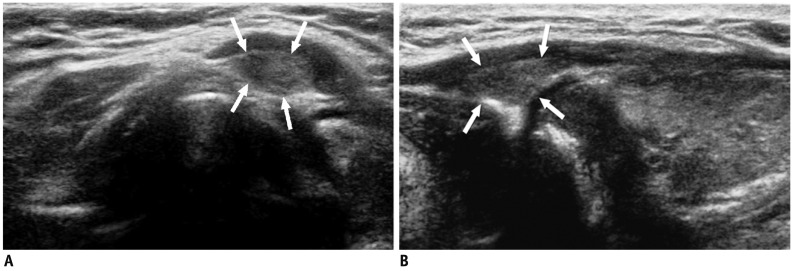
Fig. 2 Pyramidal lobe in 49-year-old woman with hypothyroidism.A. On transverse ultrasonography small isoechoic mass (arrows) was seen at superior aspect of left thyroid lobe. B. Lesion (arrows) had same echogenicity as surrounding thyroid gland; thus, providing important diagnostic clue on longitudinal view.
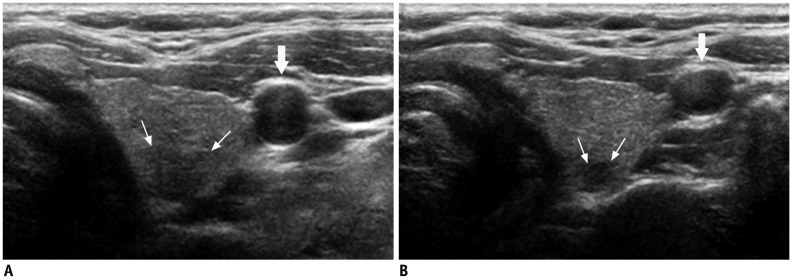
Fig. 3 Deep located lesion in left thyroid lobe in 35-year-old man.A. Without compression, ill-defined, taller-than-wide hypoechoic nodule (small arrows) suggesting suspicious nodule is visible. B. Following compression, margin of nodule can be seen more easily and carotid artery (large arrows) is also compressed.
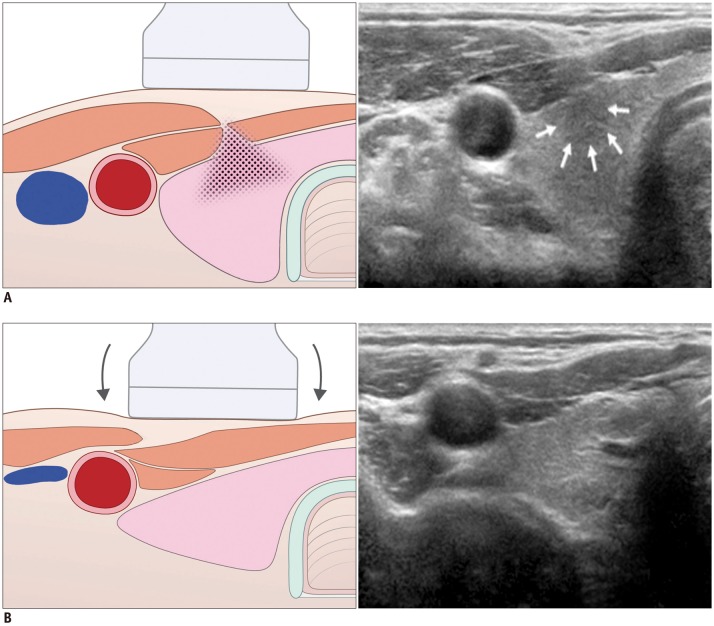
Fig. 4 Artifact related with muscle interface in 28-year-old man.A. Before compression, hypoechoic lesion (arrows) is visible in anterior portion of right thyroid lobe. B. Following compression, lesion disappeared as it was pseudo-lesion caused by shadow (field with dots) from sternocleidomastoid muscle interface.
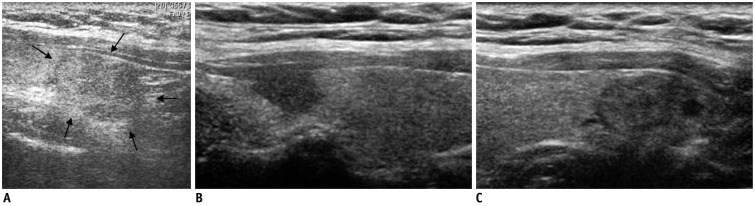
Fig. 5 Satisfaction of search in 51-year-old man with benign nodule.A. Outside ultrasonography showed nodule (arrows) in right thyroid lobe. B, C. However, another suspicious nodule was detected at tip of right upper pole. Lesion in upper pole was surgically confirmed to be papillary carcinoma, but lesion in lower pole was confirmed to be adenomatous hyperplasia.
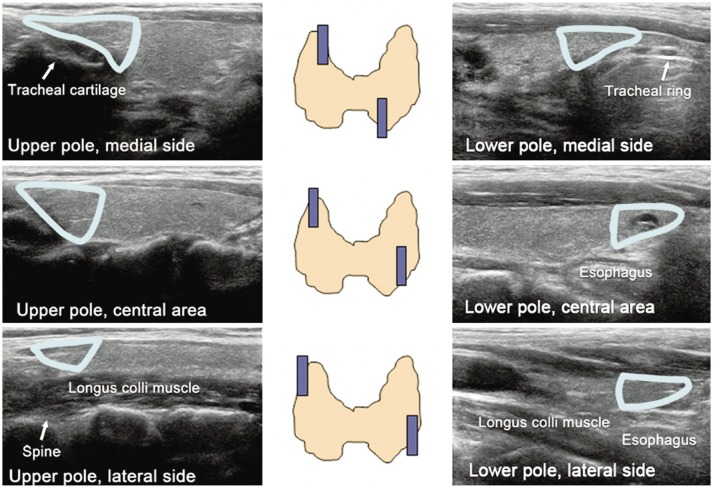
Fig. 6 Blind areas of thyroid gland on ultrasonography. Tips of thyroid gland are easily missed. It is imperative to look for triangular-shaped echogenic ends (color drawings) of both poles.
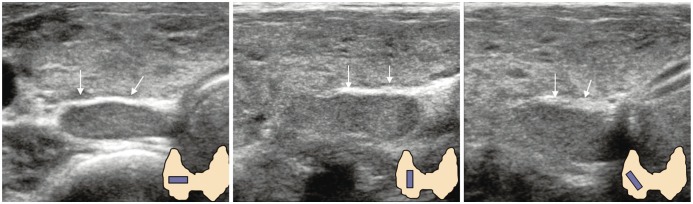
Fig. 7 Pseudo-lesion caused by posterior thyroid septum. Thyroid lobulation caused by septum (arrows) may be misdiagnosed as parathyroid lesion or thyroid nodule. In this instance, turning probe results in abrupt discontinuation of septum, and provides additional diagnostic assistance.
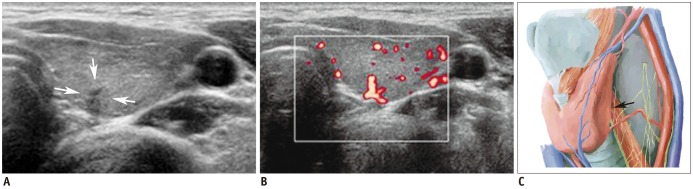
Fig. 8 Vascular structure mimicking thyroid nodule.A. Irregular, taller-than-wide, hypoechoic lesion (arrows) was seen at posterior aspect of left mid thyroid pole. B. Color Doppler scan revealed vascular structure. C. Vascular structure likely arose from inferior thyroid artery (arrow). Spectral wave form on Doppler scan would help confirmation.
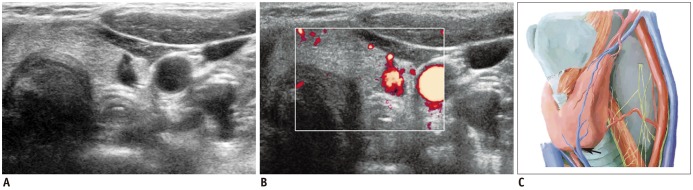
Fig. 9 Vascular structure mimicking thyroid nodule.A. Taller-than-wider lesion is visible at left lower thyroid pole. B, C. On color Doppler scan, it was proven to be vascular structure; inferior thyroid vein (arrow).
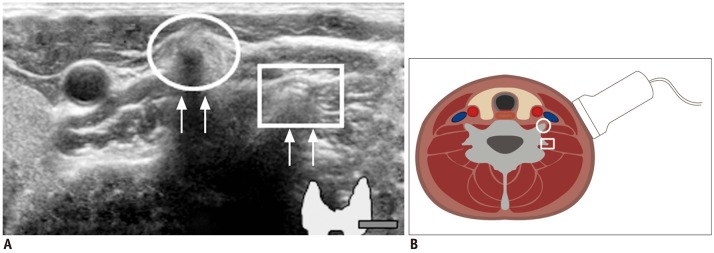
Fig. 10 Prominent vertebral transverse process mimicking calcified lymph nodes.A. Circle indicates anterior tubercle of transverse process and square identifies posterior tubercle. Echogenic line (arrows) suggested vertebral cortex. B. Sectional diagram provides more detailed explanation.
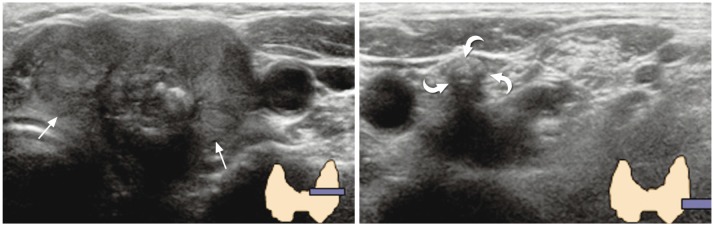
Fig. 11 Dense calcified lymph node mimicking vertebral transverse process. 69-year-old woman was referred to our hospital for diagnosed thyroid cancer (arrows). During preoperative thyroid ultrasonography, dense calcification (curved arrows) was visible at left level IV region. It was initially confused with vertebral transverse process, but was finally determined to be metastatic lymph node.
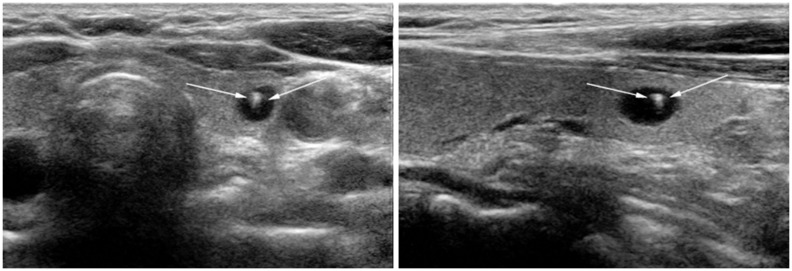
Fig. 12 Typical comet-tail artifact in benign colloid cyst. 58-year-old woman who had undergone mastectomy for breast cancer was presented for screening thyroid ultrasonography. Small cyst containing echogenic spot with comet-tail (arrows) was identified. This is typical case of "comet-tail artifact" caused by colloid crystals.
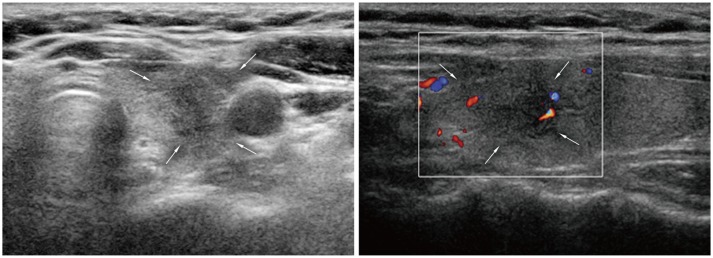
Fig. 13 Subacute thyroiditis. 48-year-old woman was referred for suspicious left thyroid lesion. Ultrasonography revealed irregular hypoechoic mass (arrows) in her left upper pole. Vascularity was noted at some peripheral areas on color Doppler imaging. Patient had experienced neck pain within past several weeks. Fine needle aspiration biopsy was performed and confirmed subacute thyroiditis.
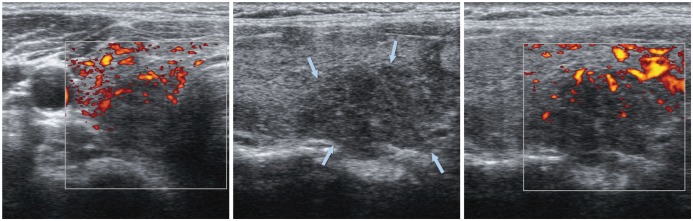
Fig. 14 Focal lymphocytic thyroiditis. 40-year-old woman underwent thyroid US for evaluation of hypothyroidism. Suspicious hypoechoic lesion (arrows) was seen in mid pole of right thyroid lobe. However, lesion was confirmed to be lymphocytic thyroiditis by US-guided fine needle aspiration biopsy. US = ultrasonography
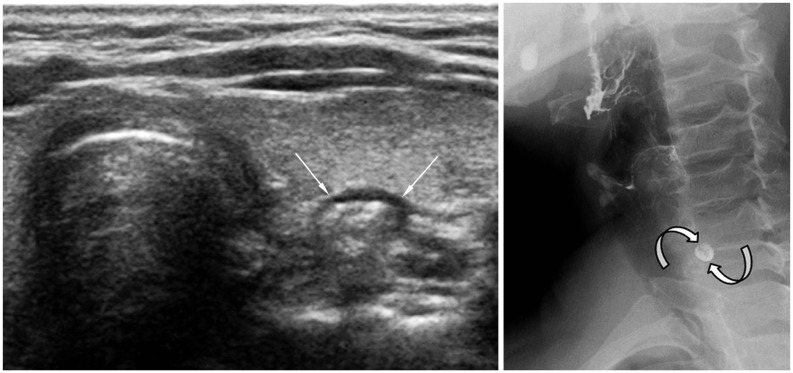
Fig. 15 Pharyngoesophageal diverticulum. 63-year-old woman was referred for evaluation of left thyroid nodule. High-resolution ultrasonography revealed pharyngoesophageal diverticulum (arrows). Small barium collection (curved arrows) suggesting diverticulum was visible on esophagography.
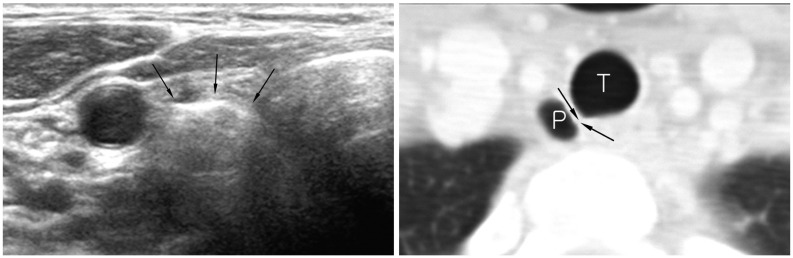
Fig. 16 Right paratracheal air cyst in 47-year-old woman. Screening ultrasonography revealed echogenic mass (arrows) suggestive of air-containing mass in right paratracheal region. Neck CT scan was performed and confirmed presence of right paratracheal air cyst with slit-like communicating channel (arrows). P = paratracheal air cyst, T = trachea
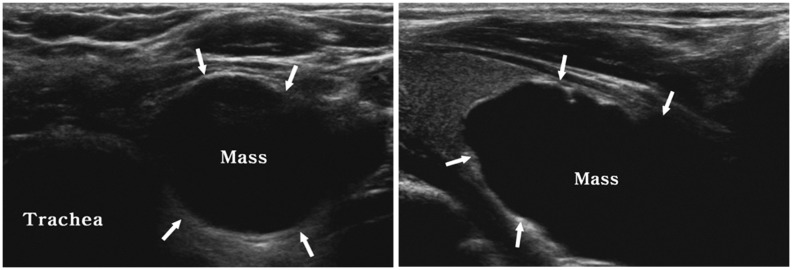
Fig. 17 Parathyroid cyst. 47-year-old woman presented with left-sided neck mass. Ultrasonography revealed large cystic mass (arrows) at inferior aspect of left thyroid lobe. Parathyroid hormone level in aspirate was 100.93 pg/mL, while thyroglobulin level was less than 0.1 ng/mL.
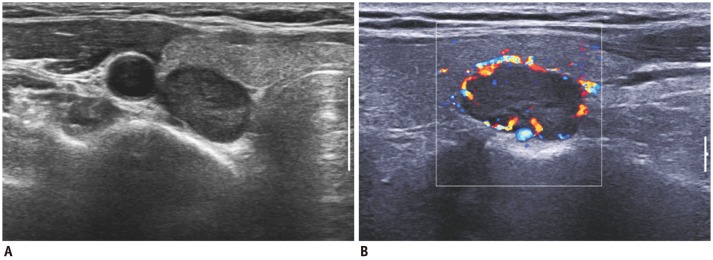
Fig. 18 Parathyroid adenoma in 54-year-old woman.A. Thyroid US revealed hypoechoic solid mass at right lower pole region. B. Color Doppler US showed characteristic peripheral vascularity. It was surgically shown to be parathyroid adenoma. US = ultrasonography
Cited by 2 articles
-
Radiofrequency versus Ethanol Ablation for Treating Predominantly Cystic Thyroid Nodules: A Randomized Clinical Trial
Jung Hwan Baek, Eun Ju Ha, Young Jun Choi, Jin Yong Sung, Jae Kyun Kim, Young Kee Shong
Korean J Radiol. 2015;16(6):1332-1340. doi: 10.3348/kjr.2015.16.6.1332.2019 Practice guidelines for thyroid core needle biopsy: a report of the Clinical Practice Guidelines Development Committee of the Korean Thyroid Association
Chan Kwon Jung, Jung Hwan Baek, Dong Gyu Na, Young Lyun Oh, Ka Hee Yi, Ho-Cheol Kang
J Pathol Transl Med. 2020;54(1):64-86. doi: 10.4132/jptm.2019.12.04.
Reference
-
1. Kim EK, Park CS, Chung WY, Oh KK, Kim DI, Lee JT, et al. New sonographic criteria for recommending fine-needle aspiration biopsy of nonpalpable solid nodules of the thyroid. AJR Am J Roentgenol. 2002; 178:687–691. PMID: 11856699.
Article2. Mazzaferri EL. Management of a solitary thyroid nodule. N Engl J Med. 1993; 328:553–559. PMID: 8426623.
Article3. Rosen IB, Azadian A, Walfish PG, Salem S, Lansdown E, Bedard YC. Ultrasound-guided fine-needle aspiration biopsy in the management of thyroid disease. Am J Surg. 1993; 166:346–349. PMID: 8214289.
Article4. Yokozawa T, Miyauchi A, Kuma K, Sugawara M. Accurate and simple method of diagnosing thyroid nodules the modified technique of ultrasound-guided fine needle aspiration biopsy. Thyroid. 1995; 5:141–145. PMID: 7647575.5. Koike E, Yamashita H, Noguchi S, Murakami T, Ohshima A, Maruta J, et al. Effect of combining ultrasonography and ultrasound-guided fine-needle aspiration biopsy findings for the diagnosis of thyroid nodules. Eur J Surg. 2001; 167:656–661. PMID: 11759733.6. Peccin S, de Castsro JA, Furlanetto TW, Furtado AP, Brasil BA, Czepielewski MA. Ultrasonography: is it useful in the diagnosis of cancer in thyroid nodules? J Endocrinol Invest. 2002; 25:39–43. PMID: 11885575.
Article7. Butch RJ, Simeone JF, Mueller PR. Thyroid and parathyroid ultrasonography. Radiol Clin North Am. 1985; 23:57–71. PMID: 3883407.8. Khati N, Adamson T, Johnson KS, Hill MC. Ultrasound of the thyroid and parathyroid glands. Ultrasound Q. 2003; 19:162–176. PMID: 14730259.
Article9. Barraclough BM, Barraclough BH. Ultrasound of the thyroid and parathyroid glands. World J Surg. 2000; 24:158–165. PMID: 10633142.
Article10. Slapa RZ, Slowinska-Srzednicka J, Szopinski KT, Jakubowski W. Gray-scale three-dimensional sonography of thyroid nodules: feasibility of the method and preliminary studies. Eur Radiol. 2006; 16:428–436. PMID: 16155720.
Article11. Hoang JK, Lee WK, Lee M, Johnson D, Farrell S. US Features of thyroid malignancy: pearls and pitfalls. Radiographics. 2007; 27:847–860. discussion 861-865. PMID: 17495296.
Article12. Kwak JY, Kim EK, Park SY, Kim MJ, Moon WJ, Choi SH, et al. Findings of extrathyroid lesions encountered with thyroid sonography. J Ultrasound Med. 2007; 26:1747–1759. PMID: 18029927.
Article13. Macdonald AJ. Diagnostic and surgical imaging anatomy. Brain, head & neck, spine. Salt Lake City: Amirsys;2006. p. II-230.14. Gritzmann N, Koischwitz D, Rettenbacher T. Sonography of the thyroid and parathyroid glands. Radiol Clin North Am. 2000; 38:1131–1145. xiiPMID: 11054973.
Article15. Desser TS, Kamaya A. Ultrasound of thyroid nodules. Neuroimaging Clin N Am. 2008; 18:463–478. viiPMID: 18656028.
Article16. Kamaya A, Quon A, Jeffrey RB. Sonography of the abnormal parathyroid gland. Ultrasound Q. 2006; 22:253–262. PMID: 17146333.
Article17. Nilsson A. Artefacts in sonography and Doppler. Eur Radiol. 2001; 11:1308–1315. PMID: 11519537.
Article18. Rumack CM, Wilson SR, Charboneau JW, Levine D. Diagnostic ultrasound. 4th ed. Philadelphia: Elsevier Mosby;2011. p. 20–21. p. 798–800.19. Stavros AT. Breast ultrasound. Philadelphia: Lippincott Williams & Wilkins;2004. p. 488–494.20. Berbaum KS, Franken EA Jr, Dorfman DD, Rooholamini SA, Kathol MH, Barloon TJ, et al. Satisfaction of search in diagnostic radiology. Invest Radiol. 1990; 25:133–140. PMID: 2312249.
Article21. Langer JE, Mandel SJ. Sonographic imaging of cervical lymph nodes in patients with thyroid cancer. Neuroimaging Clin N Am. 2008; 18:479–489. vii–viii. PMID: 18656029.
Article22. Leboulleux S, Girard E, Rose M, Travagli JP, Sabbah N, Caillou B, et al. Ultrasound criteria of malignancy for cervical lymph nodes in patients followed up for differentiated thyroid cancer. J Clin Endocrinol Metab. 2007; 92:3590–3594. PMID: 17609301.
Article23. Kuna SK, Bracic I, Tesic V, Kuna K, Herceg GH, Dodig D. Ultrasonographic differentiation of benign from malignant neck lymphadenopathy in thyroid cancer. J Ultrasound Med. 2006; 25:1531–1537. quiz 1538-1540. PMID: 17121947.
Article24. Stanley MW, Knoedler JP. Skeletal structures that clinically simulate lymph nodes: encounters during fine-needle aspiration. Diagn Cytopathol. 1993; 9:86–88. PMID: 8458291.
Article25. Papini E, Guglielmi R, Bianchini A, Crescenzi A, Taccogna S, Nardi F, et al. Risk of malignancy in nonpalpable thyroid nodules: predictive value of ultrasound and color-Doppler features. J Clin Endocrinol Metab. 2002; 87:1941–1946. PMID: 11994321.
Article26. Cappelli C, Castellano M, Pirola I, Cumetti D, Agosti B, Gandossi E, et al. The predictive value of ultrasound findings in the management of thyroid nodules. QJM. 2007; 100:29–35. PMID: 17178736.
Article27. Ito Y, Kobayashi K, Tomoda C, Uruno T, Takamura Y, Miya A, et al. Ill-defined edge on ultrasonographic examination can be a marker of aggressive characteristic of papillary thyroid microcarcinoma. World J Surg. 2005; 29:1007–1011. discussion 1011-1012. PMID: 15981041.
Article28. Cappelli C, Castellano M, Pirola I, Gandossi E, De Martino E, Cumetti D, et al. Thyroid nodule shape suggests malignancy. Eur J Endocrinol. 2006; 155:27–31. PMID: 16793946.
Article29. Moon WJ, Baek JH, Jung SL, Kim DW, Kim EK, Kim JY, et al. Ultrasonography and the ultrasound-based management of thyroid nodules: consensus statement and recommendations. Korean J Radiol. 2011; 12:1–14. PMID: 21228935.
Article30. Khoo ML, Asa SL, Witterick IJ, Freeman JL. Thyroid calcification and its association with thyroid carcinoma. Head Neck. 2002; 24:651–655. PMID: 12112538.
Article31. Ahuja A, Chick W, King W, Metreweli C. Clinical significance of the comet-tail artifact in thyroid ultrasound. J Clin Ultrasound. 1996; 24:129–133. PMID: 8838301.
Article32. Park SY, Kim EK, Kim MJ, Kim BM, Oh KK, Hong SW, et al. Ultrasonographic characteristics of subacute granulomatous thyroiditis. Korean J Radiol. 2006; 7:229–234. PMID: 17143025.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ultrasound elastography for thyroid nodules: recent advances
- Ultrasound elastography of the thyroid: principles and current status
- Effective and Safe Application of Radiofrequency Ablation for Benign Thyroid Nodules
- Ultrasonography of pediatric urogenital emergencies: review of classic and new techniques
- Sonographic Evaluation of Thyroid Nodules
