Evaluation of Femoral Tunnel Positioning Using 3-Dimensional Computed Tomography and Radiographs after Single Bundle Anterior Cruciate Ligament Reconstruction with Modified Transtibial Technique
- Affiliations
-
- 1Department of Orthopedic Surgery, JAINMEDI Hospital, Goyang, Korea.
- 2Department of Orthopedic Surgery, Chung Hospital, Seongnam, Korea.
- 3Department of Orthopedic Surgery, Inje University Seoul Paik Hospital, Seoul, Korea. boram107@hanmail.net
- KMID: 1705544
- DOI: http://doi.org/10.4055/cios.2013.5.3.188
Abstract
- BACKGROUND
The purpose of this study is to report a modified transtibial technique to approach the center of anatomical femoral footprint in anterior cruciate ligament (ACL) reconstruction and to investigate the accurate femoral tunnel position with 3-dimensional computed tomography (3D-CT) and radiography after reconstruction.
METHODS
From December 2010 to October 2011, we evaluated 98 patients who underwent primary ACL reconstruction using a modified transtibial technique to approach the center of anatomical femoral footprint in single bundle ACL reconstruction with hamstring autograft. Their femoral tunnel positions were investigated with 3D-CT and radiography postoperatively. Femoral tunnel angle was measured on the postoperative anteroposterior (AP) radiograph and the center of the femoral tunnel aperture on the lateral femoral condyle was assessed with 3D-CT according to the quadrant method by two orthopedic surgeons.
RESULTS
According to the quadrant method with 3D-CT, the femoral tunnel was measured at a mean of 32.94% +/- 5.16% from the proximal condylar surface (parallel to the Blumensaat line) and 41.89% +/- 5.58% from the notch roof (perpendicular to the Blumensaat line) with good interobserver (intraclass correlation coefficients [ICC], 0.766 and 0.793, respectively) and intraobserver reliability (ICC, 0.875 and 0.893, respectively). According to the radiographic measurement on the AP view, the femoral tunnel angles averaged 50.43degrees +/- 7.04degrees (ICC, 0.783 and 0.911, respectively).
CONCLUSIONS
Our modified transtibial technique is anticipated to provide more anatomical placement of the femoral tunnel during ACL reconstruction than the former traditional transtibial techniques.
Keyword
MeSH Terms
Figure
-
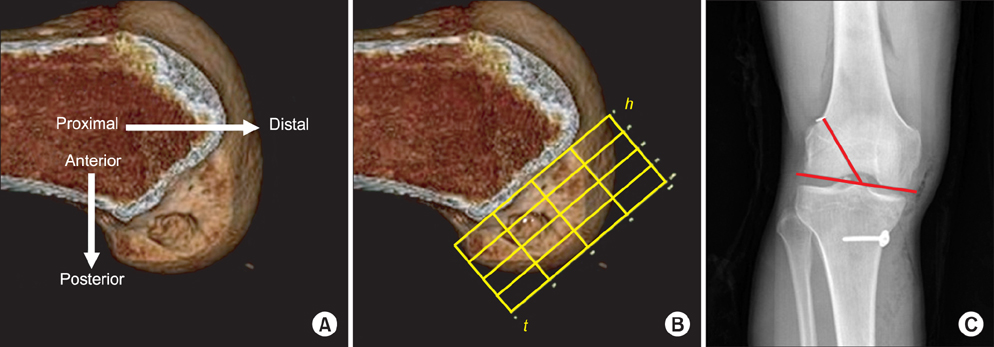
Fig. 1 (A) The medial-lateral view of the lateral femoral condyle is obtained from the 3-dimensional computed tomography, and is rotated to the strictly lateral position. (B) A rectangular measurement frame is drawn over the medial-lateral view of the lateral femoral condyle described by Bernard et al.8) (C) Lateral inclination of the femoral bone tunnel was measured with reference to a line tangent to the femoral condyle.18)
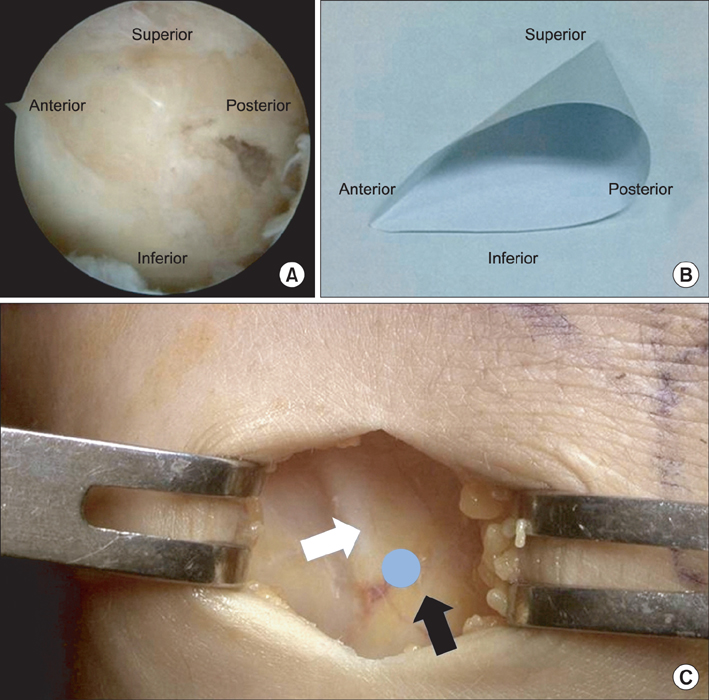
Fig. 2 (A) The triangular shaped funnel trough is made in femoral anterior cruciate ligament insertion. (B) A picture of a triangular shaped funnel model. (C) The starting point of the tibial tunnel (blue circle) is the point of interaction between lateral to anterior margin of the medial collateral ligament (white arrow) and upper margin of pes anserinus (black arrow).
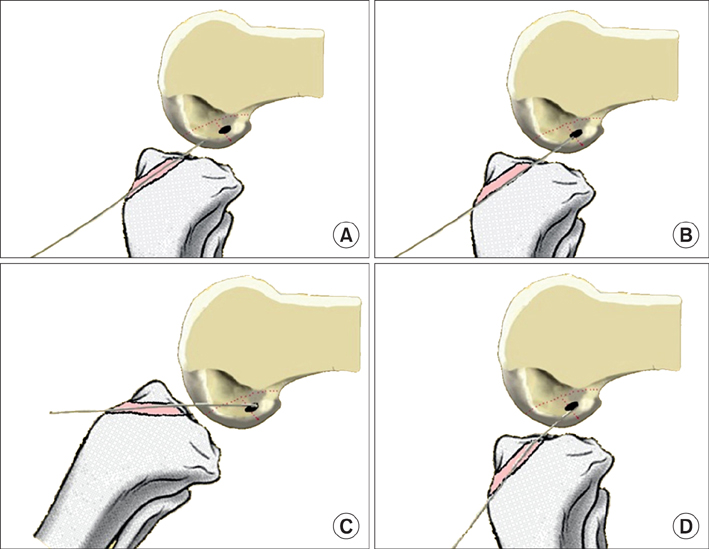
Fig. 3 (A) After creating a tibial tunnel whose size matches the diameter of the graft, the guide wire is inserted into the tibial tunnel by free-hand techniques. (B) The guide wire is inserted toward the triangular shaped funnel trough of the femur. (C) While the knee is extended gradually, the guide wire is slid into the anatomical footprint in the bony trough. (D) To prevent posterior wall blowout, the knee is flexed gradually until 90 degrees.
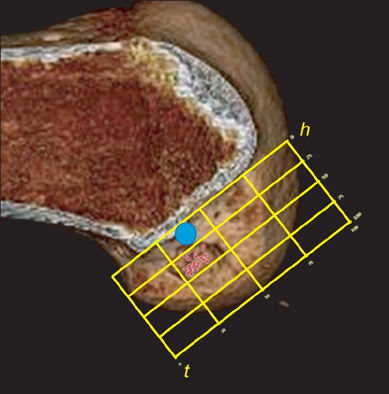
Fig. 4 Distributed mid-tunnel points of femoral tunnels according to our modified transtibial technique. Blue circle is the mid-tunnel point of femoral tunnel with traditional transtibial method.13)
Cited by 1 articles
-
Comparison of Poly-L-Lactic Acid and Poly-L-Lactic Acid/Hydroxyapatite Bioabsorbable Screws for Tibial Fixation in ACL Reconstruction: Clinical and Magnetic Resonance Imaging Results
Dhong Won Lee, Ji Whan Lee, Sang Bum Kim, Jung Ho Park, Kyu Sung Chung, Jeong Ku Ha, Jin Goo Kim, Woo Jong Kim
Clin Orthop Surg. 2017;9(3):270-279. doi: 10.4055/cios.2017.9.3.270.
Reference
-
1. Aglietti P, Giron F, Buzzi R, Biddau F, Sasso F. Anterior cruciate ligament reconstruction: bone-patellar tendon-bone compared with double semitendinosus and gracilis tendon grafts. A prospective, randomized clinical trial. J Bone Joint Surg Am. 2004; 86(10):2143–2155.2. Woo SL, Wu C, Dede O, Vercillo F, Noorani S. Biomechanics and anterior cruciate ligament reconstruction. J Orthop Surg Res. 2006; 1:2.
Article3. Loh JC, Fukuda Y, Tsuda E, Steadman RJ, Fu FH, Woo SL. Knee stability and graft function following anterior cruciate ligament reconstruction: comparison between 11 o'clock and 10 o'clock femoral tunnel placement. 2002 Richard O'Connor Award paper. Arthroscopy. 2003; 19(3):297–304.
Article4. Bedi A, Raphael B, Maderazo A, Pavlov H, Williams RJ 3rd. Transtibial versus anteromedial portal drilling for anterior cruciate ligament reconstruction: a cadaveric study of femoral tunnel length and obliquity. Arthroscopy. 2010; 26(3):342–350.
Article5. Garofalo R, Mouhsine E, Chambat P, Siegrist O. Anatomic anterior cruciate ligament reconstruction: the two-incision technique. Knee Surg Sports Traumatol Arthrosc. 2006; 14(6):510–516.
Article6. Rue JP, Ghodadra N, Bach BR Jr. Femoral tunnel placement in single-bundle anterior cruciate ligament reconstruction: a cadaveric study relating transtibial lateralized femoral tunnel position to the anteromedial and posterolateral bundle femoral origins of the anterior cruciate ligament. Am J Sports Med. 2008; 36(1):73–79.
Article7. Heming JF, Rand J, Steiner ME. Anatomical limitations of transtibial drilling in anterior cruciate ligament reconstruction. Am J Sports Med. 2007; 35(10):1708–1715.
Article8. Bernard M, Hertel P, Hornung H, Cierpinski T. Femoral insertion of the ACL: radiographic quadrant method. Am J Knee Surg. 1997; 10(1):14–21.9. Colombet P, Robinson J, Christel P, et al. Morphology of anterior cruciate ligament attachments for anatomic reconstruction: a cadaveric dissection and radiographic study. Arthroscopy. 2006; 22(9):984–992.
Article10. Tsukada H, Ishibashi Y, Tsuda E, Fukuda A, Toh S. Anatomical analysis of the anterior cruciate ligament femoral and tibial footprints. J Orthop Sci. 2008; 13(2):122–129.
Article11. Abebe ES, Moorman CT 3rd, Dziedzic TS, et al. Femoral tunnel placement during anterior cruciate ligament reconstruction: an in vivo imaging analysis comparing transtibial and 2-incision tibial tunnel-independent techniques. Am J Sports Med. 2009; 37(10):1904–1911.
Article12. Kaseta MK, DeFrate LE, Charnock BL, Sullivan RT, Garrett WE Jr. Reconstruction technique affects femoral tunnel placement in ACL reconstruction. Clin Orthop Relat Res. 2008; 466(6):1467–1474.
Article13. Kopf S, Forsythe B, Wong AK, et al. Nonanatomic tunnel position in traditional transtibial single-bundle anterior cruciate ligament reconstruction evaluated by three-dimensional computed tomography. J Bone Joint Surg Am. 2010; 92(6):1427–1431.
Article14. Miller CD, Gerdeman AC, Hart JM, et al. A comparison of 2 drilling techniques on the femoral tunnel for anterior cruciate ligament reconstruction. Arthroscopy. 2011; 27(3):372–379.
Article15. Ferretti M, Ekdahl M, Shen W, Fu FH. Osseous landmarks of the femoral attachment of the anterior cruciate ligament: an anatomic study. Arthroscopy. 2007; 23(11):1218–1225.
Article16. van Eck CF, Martins CA, Vyas SM, Celentano U, van Dijk CN, Fu FH. Femoral intercondylar notch shape and dimensions in ACL-injured patients. Knee Surg Sports Traumatol Arthrosc. 2010; 18(9):1257–1262.
Article17. Chang CB, Choi JY, Koh IJ, Lee KJ, Lee KH, Kim TK. Comparisons of femoral tunnel position and length in anterior cruciate ligament reconstruction: modified transtibial versus anteromedial portal techniques. Arthroscopy. 2011; 27(10):1389–1394.
Article18. Dargel J, Schmidt-Wiethoff R, Fischer S, Mader K, Koebke J, Schneider T. Femoral bone tunnel placement using the transtibial tunnel or the anteromedial portal in ACL reconstruction: a radiographic evaluation. Knee Surg Sports Traumatol Arthrosc. 2009; 17(3):220–227.
Article19. Piasecki DP, Bach BR Jr, Espinoza Orias AA, Verma NN. Anterior cruciate ligament reconstruction: can anatomic femoral placement be achieved with a transtibial technique? Am J Sports Med. 2011; 39(6):1306–1315.20. Dvorak MF, Fisher C, Boyd M, Johnson M, Greenhow R, Oxland TR. Anterior occiput-to-axis screw fixation: part I. A case report, description of a new technique, and anatomical feasibility analysis. Spine (Phila Pa 1976). 2003; 28(3):E54–E60.21. Saringer WF, Reddy B, Nobauer-Huhmann I, et al. Endoscopic anterior cervical foraminotomy for unilateral radiculopathy: anatomical morphometric analysis and preliminary clinical experience. J Neurosurg. 2003; 98:2 Suppl. 171–180.
Article22. Arnold MP, Kooloos J, van Kampen A. Single-incision technique misses the anatomical femoral anterior cruciate ligament insertion: a cadaver study. Knee Surg Sports Traumatol Arthrosc. 2001; 9(4):194–199.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Tomographic Study of Femoral Positioning in Anterior Cruciate Ligament Reconstruction Using the Transtibial Technique
- Femoral Tunnel Drilling Techniques in Anterior Cruciate Ligament Reconstruction
- Three-Dimensional Reconstruction Computed Tomography Evaluation of Tunnel Location during Single-Bundle Anterior Cruciate Ligament Reconstruction: A Comparison of Transtibial and 2-Incision Tibial Tunnel-Independent Techniques
- Single Bundle Anterior Cruciate Ligament Reconstruction
- Anatomical Single-bundle Anterior Cruciate Ligament Reconstruction Using a Freehand Transtibial Technique
