Spinal Meningeal Melanocytoma with Benign Histology Showing Leptomeningeal Spread: Case Report
- Affiliations
-
- 1Department of Radiology, Inje University Haeundae Paik Hospital, Busan 612-030, Korea. okkimmd@hanafos.com
- 2Department of Radiology, Inje University Busan Paik Hospital, Busan 633-165, Korea.
- 3Department of Radiology, Busan National University Hospital, Busan 602-739, Korea.
- 4Department of Pathology, Inje University Haeundae Paik Hospital, Busan 612-030, Korea.
- 5Department of Neurosurgery, Inje University Haeundae Paik Hospital, Busan 612-030, Korea.
- KMID: 1705462
- DOI: http://doi.org/10.3348/kjr.2013.14.3.470
Abstract
- Meningeal melanocytoma is a rare benign tumor with relatively good prognosis. However, local aggressive behavior of meningeal melanocytoma has been reported, especially in cases of incomplete surgical resection. Malignant transformation was raised as possible cause by prior reports to explain this phenomenon. We present an unusual case of meningeal melanocytoma associated with histologically benign leptomeningeal spread and its subsequent aggressive clinical course, and describe its radiological findings.
Keyword
MeSH Terms
Figure
-
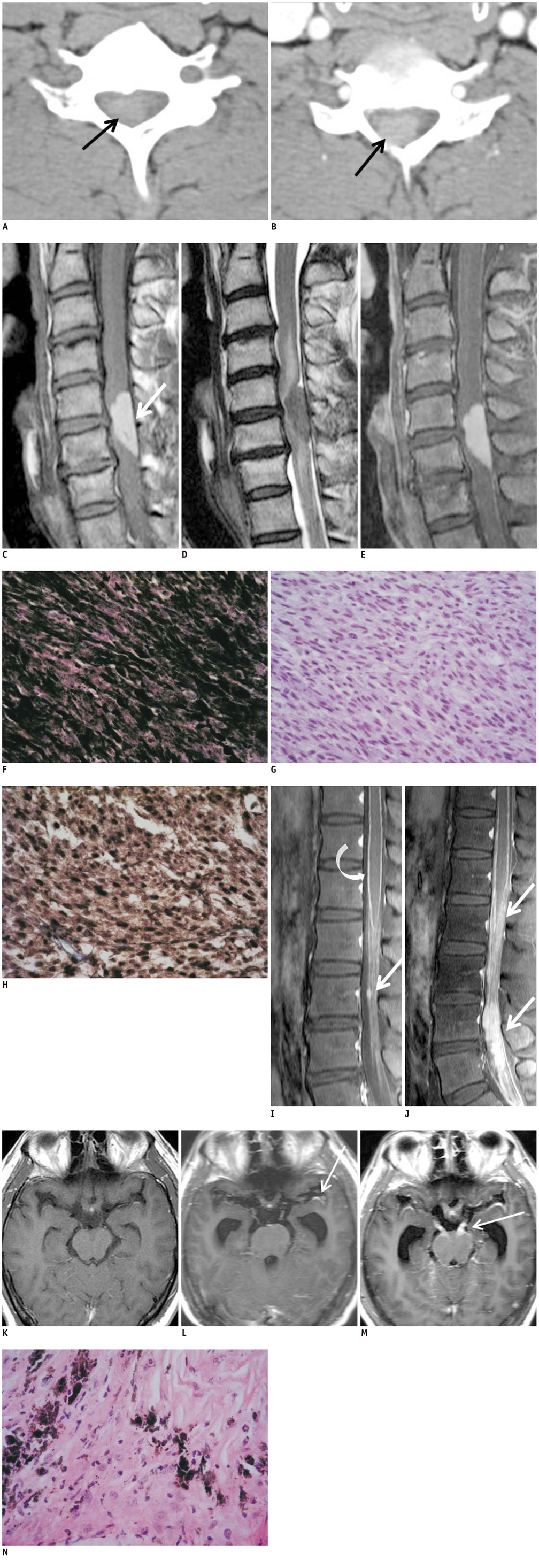
Fig. 1 Cervical meningeal melanocytoma with benign leptomeningeal spread in 37-year-old man. Cervical spinal meningeal melanocytoma in 37-year-old man. A. Non-enhanced cervical spinal CT image shows well-defined intraspinal mass (arrow) being hyperdense in relation to muscular tissue. B. Contrast-enhanced CT image shows homogeneously contrast enhancing intraspinal mass (arrow). C. Sagittal T1-weighted MR image reveals mass having homogeneous high signal intensity, which is consistent with T1-shortening effect of melanin (arrow). D. On sagittal T2-weighted image, majority of mass reveals low signal intensity and intradural extramedullary location at C5-C6. Compressed spinal cord shows intramedullary high signal intensity. E. After administration of contrast media, enhanced T1-weighted image (T1WI) shows homogeneous and strong hyperintensity of tumor. Visual assessment of degree of tumoral contrast enhancement is limited due to strong T1 hyperintensity of mass on unenhanced T1WI. Photomicrographs of cervical spinal meningeal melanocytoma from 37-year-old man. F. Microscopic examination shows tumor cells containing large amounts of melanin pigment and consequentially obscuring details of cells (H&E stain, × 400). G. After melanin bleaching, spindle cells with minimal cytologic atypia are seen (H&E stain, × 400). H. Immunohistochemical exmination shows tumor cells stained strongly positive for S-100 protein (× 400). Postoperative lumbar spinal MR images. I. Initial thoracolumbar MRI (2 weeks after first operation). Sagittal fat suppressed gadolinium enhanced T1-weighted image (T1WI) shows diffuse leptomeningeal enhancements (curved arrow) and small enhancing nodules (arrow) in cauda equina suggesting leptomeningeal spread. J. Repeated lumbar MRI (5 weeks after first operation). Sagittal fat suppressed gadolinium enhanced T1WI shows markedly extensive intraspinal masses with diffuse contrast enhancements in lumbosacral region (arrows). Postoperative brain MR images. K. Initial brain MRI (2 weeks after first operation). Axial fat supressed gadolinium enhanced T1-weighted image (T1WI) reveals no abnormal intracranial contrast enhancement or Hydrocephalus. L. Repeated brain MRI (4 weeks after first operation). Axial fat suppressed gadolinium enhanced T1WI shows newly developed hydrocephalus with mild leptomeningeal enhancements along cranial surface including left sylvian fissure (arrow), representing leptomeningeal seeding. M. Follow-up brain MRI (7 weeks after first operation). Axial fat suppressed gadolinium enhanced T1WI shows persistent hydrocephalus with diffuse leptomeningeal enhancements along cranial surfaces, brainstem and intracranial cranial nerves (arrow). N. Photomicragraph of surgical specimen of leptomeningeal seeding mass shows that mass is composed of histologically benign cells (H&E stain, × 400).
Reference
-
1. Painter TJ, Chaljub G, Sethi R, Singh H, Gelman B. Intracranial and intraspinal meningeal melanocytosis. AJNR Am J Neuroradiol. 2000. 21:1349–1353.2. Roser F, Nakamura M, Brandis A, Hans V, Vorkapic P, Samii M. Transition from meningeal melanocytoma to primary cerebral melanoma. Case report. J Neurosurg. 2004. 101:528–531.3. Wang F, Li X, Chen L, Pu X. Malignant transformation of spinal meningeal melanocytoma. Case report and review of the literature. J Neurosurg Spine. 2007. 6:451–454.4. Uozumi Y, Kawano T, Kawaguchi T, Kaneko Y, Ooasa T, Ogasawara S, et al. Malignant transformation of meningeal melanocytoma: a case report. Brain Tumor Pathol. 2003. 20:21–25.5. Bydon A, Gutierrez JA, Mahmood A. Meningeal melanocytoma: an aggressive course for a benign tumor. J Neurooncol. 2003. 64:259–263.6. Limas C, Tio FO. Meningeal melanocytoma ("melanotic meningioma"). Its melanocytic origin as revealed by electron microscopy. Cancer. 1972. 30:1286–1294.7. Chacko G, Rajshekhar V. Thoracic intramedullary melanocytoma with long-term follow-up. J Neurosurg Spine. 2008. 9:589–592.8. Chen CJ, Hsu YI, Ho YS, Hsu YH, Wang LJ, Wong YC. Intracranial meningeal melanocytoma: CT and MRI. Neuroradiology. 1997. 39:811–814.9. Brat DJ. Perry A, Brat DJ, editors. Melanocytic Neoplasm of Central Nerveous System. Practical Surgical Neuropathology: A Diagnostic Approach. 2010. Philadelphia: Churchill Livingstone;353–359.10. Clarke DB, Leblanc R, Bertrand G, Quartey GR, Snipes GJ. Meningeal melanocytoma. Report of a case and a historical comparison. J Neurosurg. 1998. 88:116–121.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Primary Spinal Meningeal Melanocytoma
- Primary Meningeal Melanocytoma in the Thoracic Spine: A Case Report
- Meningeal Melanocytoma Associated with Ota's Nevus: Report of a case
- Spinal meningeal melanocytoma
- Primary Intramedullary Meningeal Melanocytoma in Cervical Spine: A Case Report and Literature Review
