J Educ Eval Health Prof.
2006;3:3.
The Future of e-Learning in Medical Education: Current Trend and Future Opportunity
- Affiliations
-
- 1Department of Family Medicine and Department of Medical Education and Biomedical Informatics, School of Medicine, University of Washington, Box 356390 Seattle, WA 98195-7230, U.S.A. sarakim@u.washington.edu
Abstract
- A wide range of e-learning modalities are widely integrated in medical education. However, some of the key questions related to the role of e-learning remain unanswered, such as (1) what is an effective approach to integrating technology into pre-clinical vs. clinical training?; (2) what evidence exists regarding the type and format of e-learning technology suitable for medical specialties and clinical settings?; (3) which design features are known to be effective in designing on-line patient simulation cases, tutorials, or clinical exams?; and (4) what guidelines exist for determining an appropriate blend of instructional strategies, including on-line learning, face-to-face instruction, and performance-based skill practices? Based on the existing literature and a variety of e-learning examples of synchronous learning tools and simulation technology, this paper addresses the following three questions: (1) what is the current trend of e-learning in medical education?; (2) what do we know about the effective use of e-learning?; and (3) what is the role of e-learning in facilitating newly emerging competency-based training? As e-learning continues to be widely integrated in training future physicians, it is critical that our efforts in conducting evaluative studies should target specific e-learning features that can best mediate intended learning goals and objectives. Without an evolving knowledge base on how best to design e-learning applications, the gap between what we know about technology use and how we deploy e-learning in training settings will continue to widen.
MeSH Terms
Figure
-
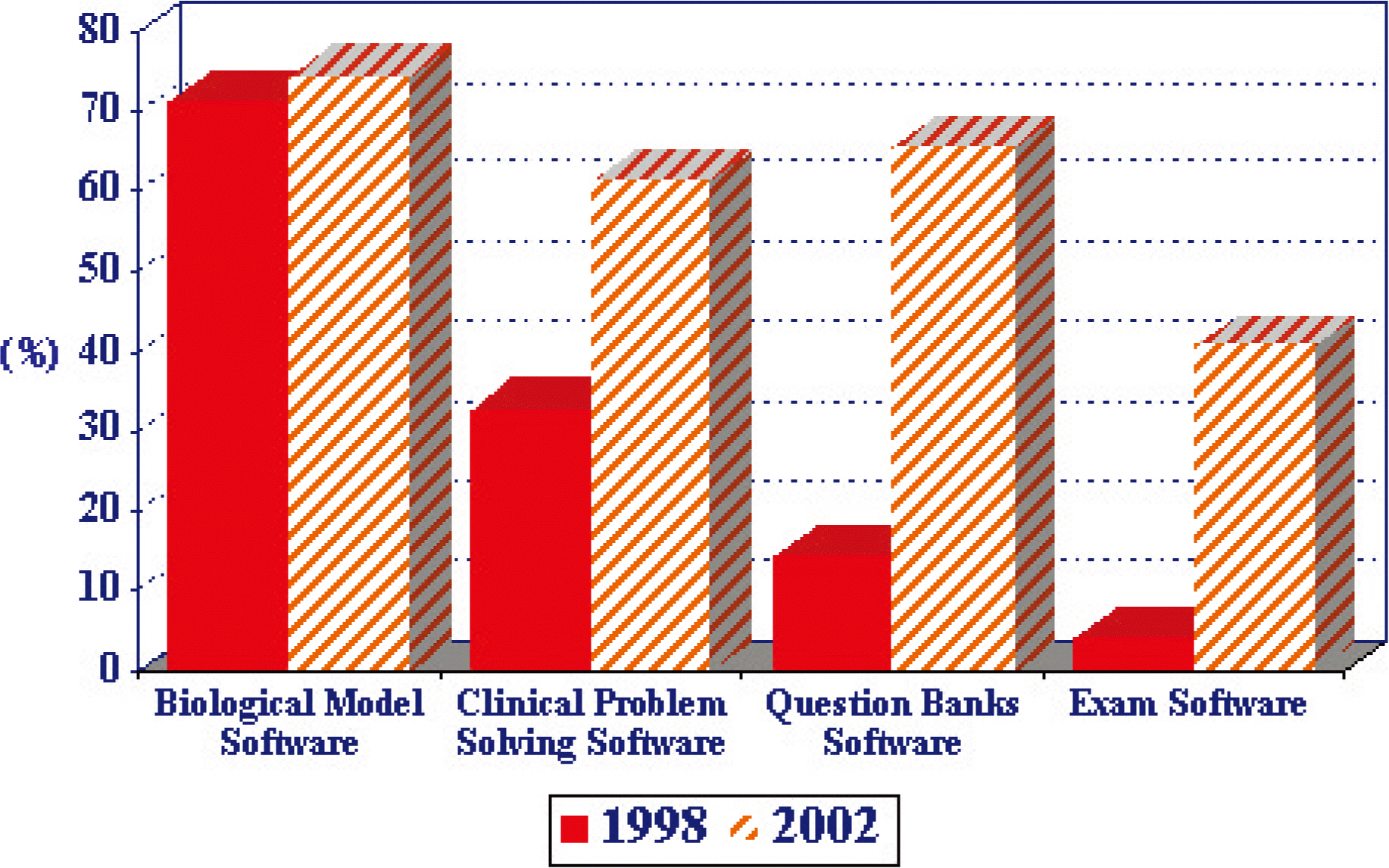
Fig. 1. Comparison of percentages of 125 US medical schools reporting the use of eductional software program in basic sciences curriculum in 1998 and 2002.
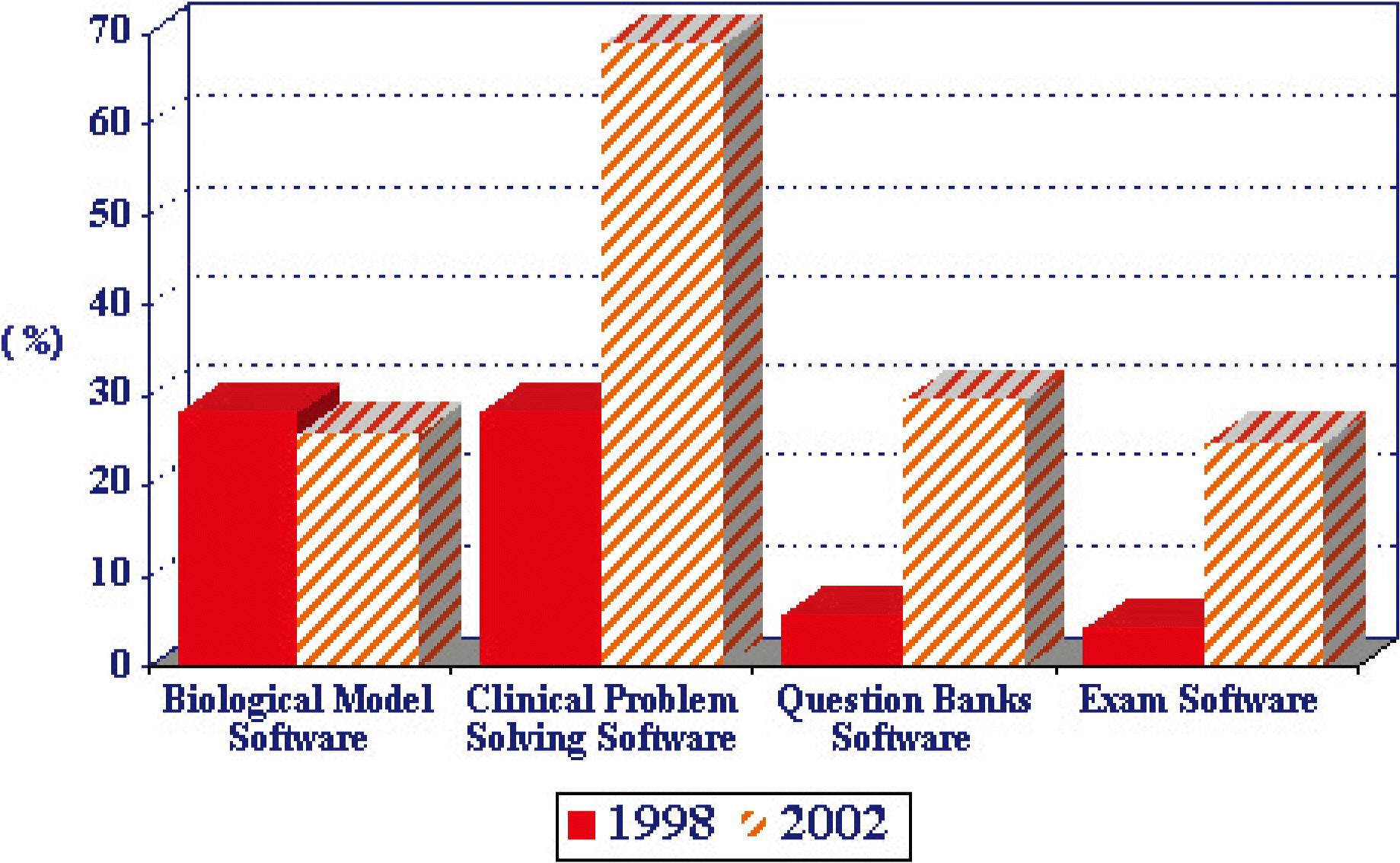
Fig. 2. Comparison of percentages of 125 US medical schools reporting the use of eductional software program in clinical clerkships in 1998 and 2002.
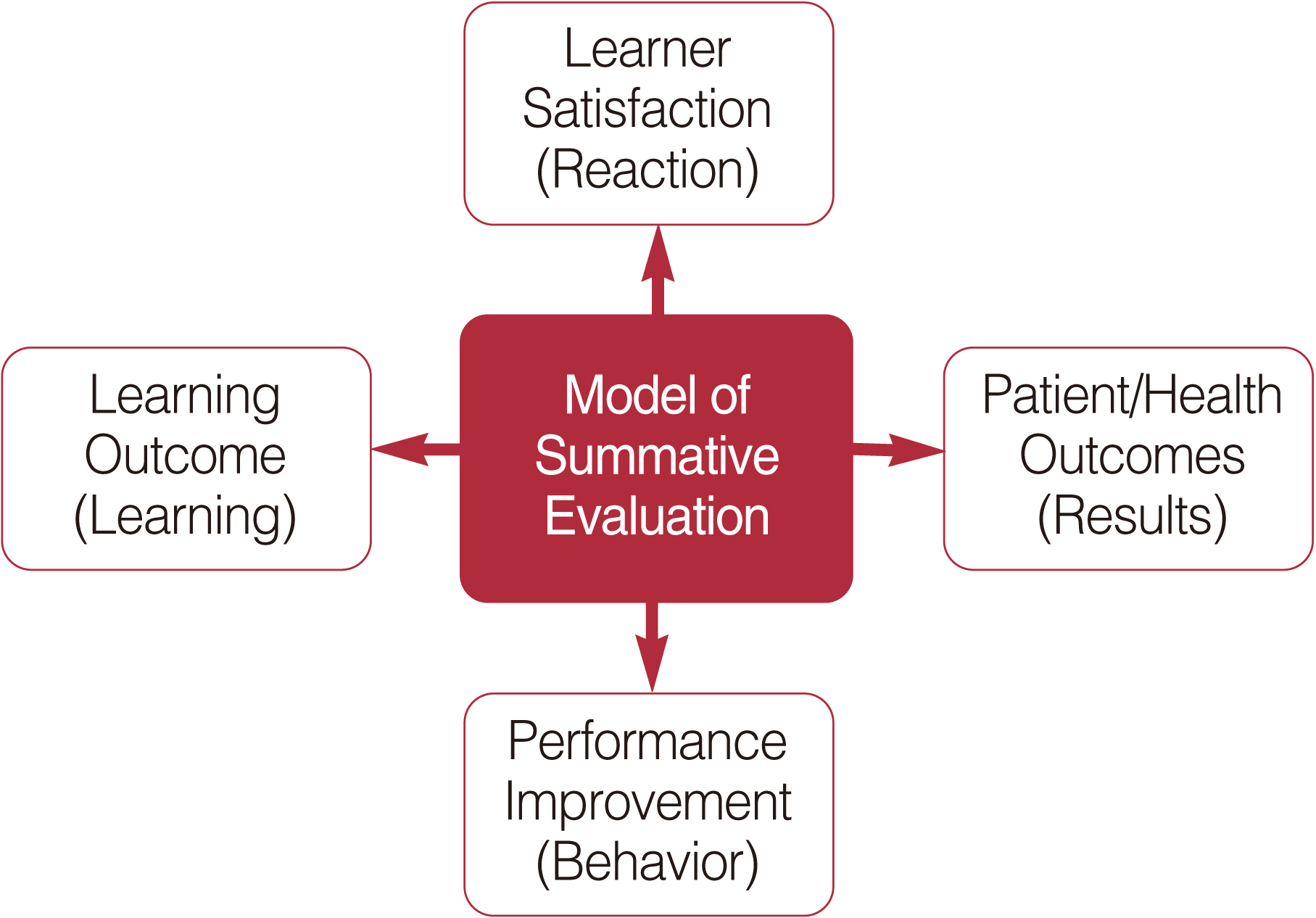
Fig. 3. Kirkpatrick s model of summative evaluation.
Reference
-
1. The Ad Hoc Committee of Deans. Educating doctors to provide high quality medical care: a vision for medical education in the United States [Internet]. Washington, DC: Association of American Medical Colleges;c2004. [cited 2006 Jul 20]. Available from: https://services.aamc.org/Publications/showfile.cfm?file=version27.pdf&prd_id=115&prv_id=130&pdf_id=27.2. Whitcomb ME. More on competency-based education. Acad Med. 2004; 79:493–4.
Article3. Ruiz JG, Mintzer MJ, Leipzig RM. The impact of E-learning in medical education. Acad Med. 2006; 81:207–12.
Article4. McKimm J, Jollie C, Cantillon P. ABC of learning and teaching: Web based learning. BMJ. 2003; 326:870–3.
Article5. Smith SR. Is there a Virtual Medical School on the horizon. Med Health R I. 2003; 86:272–5.6. Walsh K. Blended learning. BMJ. 2005; 330:829.
Article7. Lau F, Bates J. A review of e-learning practices for undergraduate medical education. J Med Syst. 2004; 28:71–87.
Article8. Moberg TF, Whitcomb ME. Educational technology to facilitate medical students’ learning: background paper 2 of the medical school objectives project. Acad Med. 1999; 74:1146–50.9. Curran VR, Fleet L. A review of evaluation outcomes of web-based continuing medical education. Med Educ. 2005; Jun. 39(6):561–7.
Article10. Bell DS, Fonarow GC, Hays RD, Mangione CM. Self-study from web-based and printed guideline materials. A randomized, controlled trial among resident physicians. Ann Intern Med. 2000; 132:938–46.11. Cook DA, Dupras DM, Thompson WG, Pankratz VS. Web-based learning in residents’ continuity clinics: a randomized, controlled trial. Acad Med. 2005; 80:90–7.
Article12. Kirkpatrick DL. Evaluating training programs: the four levels. San Francisco: Berrett-Koehler;1994.13. Adler MD, Johnson KB. Quantifying the literature of computer-aided instruction in medical education. Acad Med. 2000; 75:1025–8.
Article14. Chumley-Jones HS, Dobbie A, Alford CL. Web-based learning: sound educational method or hype? A review of the evaluation literature. Acad Med. 2002; 77(10 Suppl):S86–93.15. Letterie GS. Medical education as a science: the quality of evidence for computer-assisted instruction. Am J Obstet Gynecol. 2003; 188:849–53.
Article16. Issenberg SB, McGaghie WC, Petrusa ER, Lee Gordon D, Scalese RJ. Features and uses of high-fidelity medical simulations that lead to effective learning: a BEME systematic review. Med Teach. 2005; 27:10–28.17. Whitcomb ME. More on improving the education of doctors. Acad Med. 2003; 78:349–50.
Article18. Clever SL, Novack DH, Cohen DG, Levinson W. Evaluating surgeons’ informed decision making skills: pilot test using a videoconferenced standardised patient. Med Educ. 2003; 37:1094–9.
Article19. Chan DK, Gallagher TH, Reznick R, Levinson W. How surgeons disclose medical errors to patients: a study using standardized patients. Surgery. 2005; 138:851–8.
Article20. Novack DH, Cohen D, Peitzman SJ, Beadenkopf S, Gracely E, Morris J. A pilot test of WebOSCE: a system for assessing trainees’ clinical skills via teleconference. Med Teach. 2002; 24:483–7.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Future of Flexible Learning and Emerging Technology in Medical Education: Reflections from the COVID‐19 Pandemic
- Evaluation of Premedical Curriculum at Korea University
- Elective Course in Undergraduate Medical Education in Korea : Issues and Prospectives
- Faculty perceptions and use of e-learning resources for medical education and future predictions
- Deep Learning in Nuclear Medicine and Molecular Imaging: Current Perspectives and Future Directions
