Thyroid Dysfunction Induced by Metastatic Thyroid Cancer: Report of Two Cases
- Affiliations
-
- 1Department of Endocrinology and Metabolism, Pusan National University, Busan, Korea. injkim@pusan.ac.kr
- 2Department of Endocrinology and Metabolism, Kim Yong Ki Internal Medicine Clinic, Busan, Korea.
- KMID: 1497765
- DOI: http://doi.org/10.3803/EnM.2010.25.4.370
Abstract
- Metastases to the thyroid gland are not frequently observed in clinical practice, although an overall incidence of secondary thyroid malignant tumors has been reported to range from 1.25% to 24% in autopsy series. Generally, patients with metastatic thyroid cancer present with euthyroidism and they do not develop thyroid dysfunction. Thyroid dysfunctions, including hypothyroidism and hyperthyroidism, rarely occur in patients with metastatic thyroid cancer. We describe here a case of hypothyroidism induced by thyroid metastasis from cancer of an unknown primary site in a 53-year-old man and another case of thyrotoxicosis induced by thyroid metastasis from lung cancer in a 65-year-old man.
Keyword
MeSH Terms
Figure
-
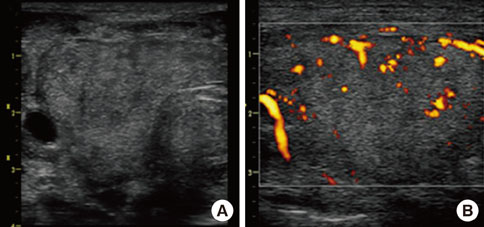
Fig. 1 (A) Ultrasonographic findings. Both lobes of the thyroid gland are enlarged with the heterogeneous echogenicity of the parenchyma and scattered hypoechoic areas. (B) Color Doppler shows that blood flow is slightly decreased in the parenchyma of both glands.
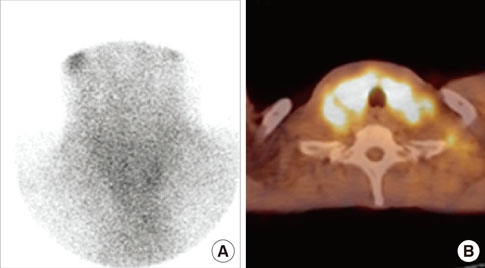
Fig. 2 (A) TcO4-99m thyroid scan. The thyroid gland is poorly visualized. (B) F(18)-FDG PET/CT image demonstrates increased FDG uptake (maxSUV: right, 5.4; left, 5.1) in the thyroid gland and paratracheal LN (maxSUV: 4.7).

Fig. 3 Histologic findings. (A) Cytologic examination of fine needle aspirates from the thyroid gland reveals adenocarcinoma, most likely metastatic, with frequent papillary growth (H&E, × 200). (B) Cytologic examination of fine needle aspirates from the thyroid gland exhibits squamous cell carcinoma (H&E, × 400).
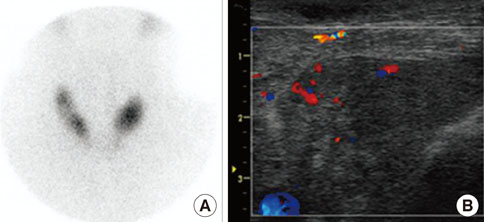
Fig. 4 (A) TcO4-99m thyroid scan. Both lobes of the thyroid gland have a cold space occupying lesion (SOL). (B) Ultrasonographic findings. Diffuse and focal hypoechogenicities are seen on both lobes.
Reference
-
1. Mortensen J, Woolner LB, Bennett WA. Secondary malignant tumors of the thyroid gland. Cancer. 1956. 9:306–309.2. Lam KY, Lo CY. Metastatic tumors of the thyroid gland: a study of 79 cases in Chinese patients. Arch Pathol Lab Med. 1998. 122:37–41.3. Shimaoka K, Sokal JE, Pickren JW. Metastatic neoplasms in the thyroid gland: pathological and clinical findings. Cancer. 1962. 15:557–565.4. Wood K, Vini L, Harmer C. Metastases to the thyroid gland: the Royal Marsden experience. Eur J Surg Oncol. 2004. 30:583–588.5. Kim TY, Kim WB, Gong G, Hong SJ, Shong YK. Metastasis to the thyroid diagnosed by fine-needle aspiration biopsy. Clin Endocrinol (Oxf). 2005. 62:236–241.6. Nakhjavani MK, Gharib H, Goellner JR, van Heerden JA. Metastasis to the thyroid gland. A report of 43 cases. Cancer. 1997. 79:574–578.7. Hull OH. Critical analysis of two hundred twenty-one thyroid glands; study of thyroid glands obtained at necropsy in Colorado. AMA Arch Pathol. 1955. 59:291–311.8. Abrams HL, Spiro R, Goldstein N. Metastases in carcinoma; analysis of 1,000 autopsied cases. Cancer. 1950. 3:74–85.9. Wychulis AR, Beahrs OH, Woolner LB. Metastasis of carcinoma to the thyroid gland. Ann Surg. 1964. 160:169–177.10. McCabe DP, Farrar WB, Petkov TM, Finkelmeier W, O'Dwyer P, James A. Clinical and pathologic correlations in disease metastatic to the thyroid gland. Am J Surg. 1985. 150:519–523.11. Papi G, Corrado S, Scaltriti L, Carapezzi C, Ezzat S. Metastasis of urothelial sarcomatoid carcinoma to a toxic multinodular goiter. Endocr Pathol. 2005. 16:153–156.12. Eriksson M, Ajmani SK, Mallette LE. Hyperthyroidism from thyroid metastasis of pancreatic adenocarcinoma. JAMA. 1977. 238:1276–1278.13. Papi G, Fadda G, Corsello SM, Corrado S, Rossi ED, Radighieri E, Miraglia A, Carani C, Pontecorvi A. Metastases to the thyroid gland: prevalence, clinicopathological aspects and prognosis: a 10-year experience. Clin Endocrinol (Oxf). 2007. 66:565–571.14. Bae WK, Shim HJ, Choi YD, Kim JW, Cho SH, Kang HC, Chung IJ. Severe hypothyroidism induced by thyroid metastasis of cholangiocarcinoma. Cancer Res Treat. 2009. 41:56–58.15. Miyakawa M, Sato K, Hasegawa M, Nagai A, Sawada T, Tsushima T, Takano K. Severe thyrotoxicosis induced by thyroid metastasis of lung adenocarcinoma: a case report and review of the literature. Thyroid. 2001. 11:883–888.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Concurrent Primary Carcinoma and Metastatic Lesions of the Thyroid
- An Unusual Case of Metastatic Non-Small Cell Lung Cancer Misidentified as Anaplastic Thyroid Cancer
- Preoperative Staging of Well Differentiated Thyroid Cancer: US Is Enough?
- Giant Thyroid Cancer in Elderly Patient
- Thyroid Dysfunction in the Elderly
