Clinical Results of Various Surgical Techniques for Isolated Fracture of Greater Tuberosity of Humerus
- Affiliations
-
- 1Department of Orthopaedic Surgery, Kyung Hee University Hospital at Gangdong, College of Medicine, Kyung Hee University, Seoul, Korea.
- 2Department of Orthopaedic Surgery, Kyung Hee University Hospital, College of Medicine, Kyung Hee University, Seoul, Korea. shoulderrhee@hanmail.net
- KMID: 1496168
- DOI: http://doi.org/10.12671/jkfs.2013.26.2.133
Abstract
- PURPOSE
To compare the clinical and radiologic outcomes of various surgical techniques for an isolated fracture of greater tuberosity of the humerus.
MATERIALS AND METHODS
From February 2001 to December 2008, 31 patients, who underwent an operation for isolated greater tuberosity fracture and were followed up for more than 1 year, were enrolled in this study. The mean age at the time of operation was 49.3 years (range, 23-73 years). The operation methods included in this study were as follows: a transosseous suture using nonabsorbable suture material (16 cases), a fixation by cannulated screws (10 cases), tension band wiring (2 cases), bony fragment excision with rotator cuff repair (2 cases), and percutaneous pinning (1 case).
RESULTS
At the last follow-up, the average Constant score was 79.4 and Korean Shoulder Score (KSS) was 81.2. Among the various operation methods used in this study, the transosseous suture had the highest scores with 82.5 in Constant score and 89.3 in KSS. Bone union was achieved at average 10.3 weeks (range, 7-15 weeks), and there were 2 cases in which the reoperation was required due to internal fixation failure. Postoperative shoulder stiffness occurred in 3 cases, and all the cases were done with the deltopectoral approach.
CONCLUSION
Clinically and radiologically satisfactory results were obtained using various operation techniques for an isolated greater tuberosity fracture of the humerus. The transosseous suture showed relatively better results than the other methods used in this study. To achieve favorable clinical and radiologic results, it is important to select an appropriate surgical approach and fixation method according to the fracture site, degree of displacement, and size of fragment.
Keyword
MeSH Terms
Figure
-

Fig. 1 (A) Right shoulder antero-posterior view shows isolated humerus greater tuberosity fracture of a 36 years old female patient. (B) Immediate postoperative radiograph shows the acceptable reduction and fixation by transosseous sutures. (C) Eight months later, radiograph shows that complete bone union was achieved.
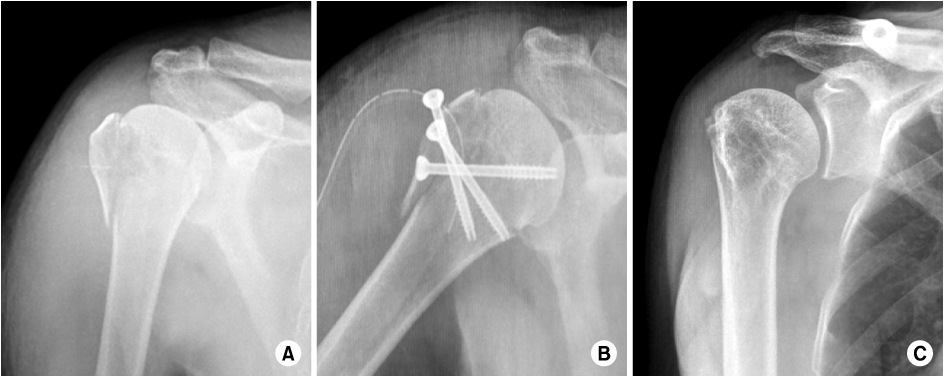
Fig. 2 (A) Right shoulder antero-posterior view of a 53 years old male patient shows isolated humerus greater tuberosity fracture with mild displacement. (B) Immediate postoperative radiograph shows satisfactory anatomical reduction and fixation by multiple cannulated screws. (C) Twelve months after surgery, radiograph shows that complete bone union was obtained.
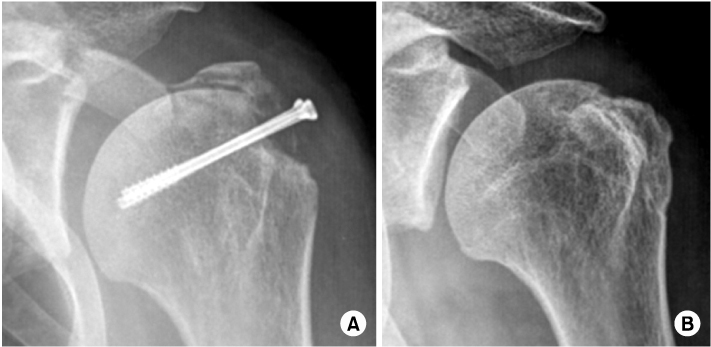
Fig. 3 (A) Left shoulder antero-posterior view of a 51 years old female patient shows reduction failure after fixation by two cannulated screws for isolated humerus greater tuberosity fracture. (B) Seven months after the revision surgery, radiograph shows that complete bone union was obtained.
Reference
-
1. Bahrs C, Lingenfelter E, Fischer F, Walters EM, Schnabel M. Mechanism of injury and morphology of the greater tuberosity fracture. J Shoulder Elbow Surg. 2006. 15:140–147.
Article2. Cornell CN, Levine D, Pagnani MJ. Internal fixation of proximal humerus fractures using the screw-tension band technique. J Orthop Trauma. 1994. 8:23–27.
Article3. Court-Brown CM, Garg A, McQueen MM. The epidemiology of proximal humeral fractures. Acta Orthop Scand. 2001. 72:365–371.
Article4. Court-Brown CM, Garg A, McQueen MM. The translated two-part fracture of the proximal humerus. Epidemiology and outcome in the older patient. J Bone Joint Surg Br. 2001. 83:799–804.5. Crichlow RJ, Andres PL, Morrison SM, Haley SM, Vrahas MS. Depression in orthopaedic trauma patients. Prevalence and severity. J Bone Joint Surg Am. 2006. 88:1927–1933.
Article6. Fenichel I, Oran A, Burstein G, Perry Pritsch M. Percutaneous pinning using threaded pins as a treatment option for unstable two- and three-part fractures of the proximal humerus: a retrospective study. Int Orthop. 2006. 30:153–157.
Article7. Flatow EL, Cuomo F, Maday MG, Miller SR, McIlveen SJ, Bigliani LU. Open reduction and internal fixation of two-part displaced fractures of the greater tuberosity of the proximal part of the humerus. J Bone Joint Surg Am. 1991. 73:1213–1218.
Article8. Green A, Izzi J Jr. Isolated fractures of the greater tuberosity of the proximal humerus. J Shoulder Elbow Surg. 2003. 12:641–649.
Article9. Hall MC, Rosser M. The structure of the upper end of the humerus with reference to osteoporotic changes in senescence leading to fractures. Can Med Assoc J. 1963. 88:290–294.10. Horak J, Nilsson BE. Epidemiology of fracture of the upper end of the humerus. Clin Orthop Relat Res. 1975. (112):250–253.
Article11. Johnson JR, Bayley JI. Early complications of acute anterior dislocation of the shoulder in the middle-aged and elderly patient. Injury. 1982. 13:431–434.
Article12. Konrad GG, Mehlhorn A, Kühle J, Strohm PC, Südkamp NP. Proximal humerus fractures-current treatment options. Acta Chir Orthop Traumatol Cech. 2008. 75:413–421.13. Kristiansen B, Christensen SW. Proximal humeral fractures Late results in relation to classification and treatment. Acta Orthop Scand. 1987. 58:124–127.
Article14. McLaughlin HL. dislocation of the shoulder with tuberosity fracture. Surg Clin North Am. 1963. 43:1615–1620.
Article15. Neer CS 2nd. Displaced proximal humeral fractures. I. Classification and evaluation. J Bone Joint Surg Am. 1970. 52:1077–1089.16. Neer CS 2nd. Displaced proximal humeral fractures. II. Treatment of three-part and four-part displacement. J Bone Joint Surg Am. 1970. 52:1090–1103.17. Park MC, Murthi AM, Roth NS, Blaine TA, Levine WN, Bigliani LU. Two-part and three-part fractures of the proximal humerus treated with suture fixation. J Orthop Trauma. 2003. 17:319–325.
Article18. Resch H, Hübner C, Schwaiger R. Minimally invasive reduction and osteosynthesis of articular fractures of the humeral head. Injury. 2001. 32:Suppl 1. SA25–SA32.
Article19. Siegel JA, Dines DM. Techniques in managing proximal humeral malunions. J Shoulder Elbow Surg. 2003. 12:69–78.
Article20. Taverna E, Sansone V, Battistella F. Arthroscopic treatment for greater tuberosity fractures: rationale and surgical technique. Arthroscopy. 2004. 20:e53–e57.
Article21. Wheeler DL, Colville MR. Biomechanical comparison of intramedullary and percutaneous pin fixation for proximal humeral fracture fixation. J Orthop Trauma. 1997. 11:363–367.
Article22. Williams GR Jr, Wong KL. Two-part and three-part fractures: open reduction and internal fixation versus closed reduction and percutaneous pinning. Orthop Clin North Am. 2000. 31:1–21.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Isolated Avulsion Fracture of the Lesser Tuberosity of the Humerus: A Case Report
- Analysis of Risk Factors for Occult Surgical Neck Fracture Accompanying Isolated Greater Tuberosity Fracture of Humerus
- The Surgical Outcomes of Isolated Greater Tuberosity Fractures of the Proximal Humerus Fixed with the Spring Plate
- Shoulder Quadruple Dislocation Fracture: Fracture of Glenoid Rim, Coracoid Process, Greater Tuberosity, Surgical Neck of Humerus Associated with Anterior Shoulder Dislocation: A Case Report
- Radiologic assessment of the displacement of the greater tuberosity of the humerus
