Diagnosis of Incomplete Kawasaki Disease in Infants Based on an Inflammation at the Bacille Calmette-Guerin Inoculation Site
- Affiliations
-
- 1Department of Pediatrics, College of Medicine, University of Ulsan, Seoul, Korea. pediatrist@medimail.co.kr
- 2Department of Pediatrics, Kosin University Gospel Hospital, Busan, Korea.
- KMID: 1491098
- DOI: http://doi.org/10.4070/kcj.2012.42.12.823
Abstract
- BACKGROUND AND OBJECTIVES
This study was intended to test how the inflammation at the Bacille Calmette-Guerin (BCG) inoculation site (BCGitis) can be a useful a diagnostic feature of Kawasaki disease (KD).
SUBJECTS AND METHODS
All subjects were infants at the time of admission, and had received BCG vaccination during their neonatal period. There were 54 patients with complete KD (group 1) and 29 patients with incomplete KD (group 2). All 83 patients had BCGitis during the acute phase of illness. Data regarding the coronary artery diameters in 31 age-matched controls were used for comparison.
RESULTS
The 2 patient groups did not differ in clinical and laboratory variables. During the acute phase, the median z scores of the left anterior descending coronary artery (LAD) diameter were 0.20, 0.42, and -0.48 in groups 1, 2, and control respectively, and that of right coronary artery (RCA) diameters were -0.15, -0.16, and -1.17 respectively. The z scores in both patient groups were greater than those in controls (p=0.0014 in LAD and p<0.0001 in RCA between group 1 and controls; p=0.0023 in LAD and p<0.0001 in RCA between group 2 and controls). A similar pattern was observed during the subacute and convalescent phases.
CONCLUSION
BCGitis is a useful feature in the diagnosis of incomplete KD in infants who received BCG vaccine during neonatal period.
MeSH Terms
Figure
-
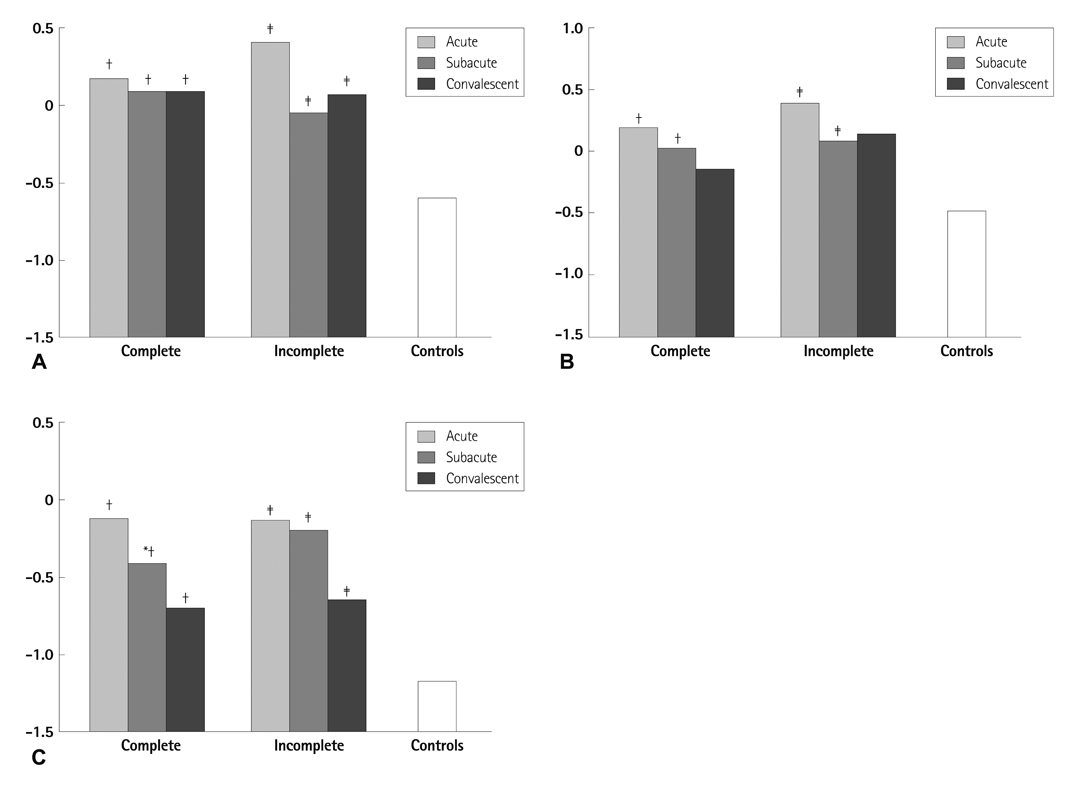
Fig. 1 Z-scores of the diameters of coronary arteries (left main coronary artery in A, left anterior descending artery in B, and right coronary artery in C) during 3 phases of illness. *p<0.05, complete presentation group vs. incomplete presentation group, †p<0.05, complete presentation group vs. controls, ‡p<0.05, incomplete presentation group vs. controls.

Fig. 2 Flow diagram of the application of the American Heart Asscociation (AHA) algorithm in patients with incomplete Kawasaki disease (KD). CRP: Creactive protein, ESR: erythrocyte sedimentation rate, Echo: echocardiography, OR: odds ratio.
Cited by 1 articles
-
Clinical Significance of the Bacille Calmette-Guérin Site Reaction in Kawasaki Disease Patients Aged Less than 18 Months
Sung Hyeon Park, Jeong Jin Yu, Jihye You, Mi Jin Kim, Eun Jung Shin, Hyun Ok Jun, Jae Suk Baek, Young-Hwue Kim, Jae-Kon Ko
Pediatr Infect Vaccine. 2018;25(3):148-155. doi: 10.14776/piv.2018.25.e11.
Reference
-
1. Ayusawa M, Sonobe T, Uemura S, et al. Revision of diagnostic guidelines for Kawasaki disease (the 5th revised edition). Pediatr Int. 2005. 47:232–234.2. Newburger JW, Takahashi M, Gerber MA, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation. 2004. 110:2747–2771.3. Sonobe T, Kiyosawa N, Tsuchiya K, et al. Prevalence of coronary artery abnormality in incomplete Kawasaki disease. Pediatr Int. 2007. 49:421–426.4. Witt MT, Minich LL, Bohnsack JF, Young PC. Kawasaki disease: more patients are being diagnosed who do not meet American Heart Association criteria. Pediatrics. 1999. 104:e10.5. Cho MA, Choi YJ, Jung JW. Affects of "age at diagnosis" on coronary artery lesions in patients with incomplete kawasaki disease. Korean Circ J. 2010. 40:283–287.6. Lee HJ. Classification of vaccination and immunization schedule recommended by the Korean Pediatric Society, 2008. J Korean Med Assoc. 2008. 51:104–109.7. Chalmers D, Corban JG, Moore PP. BCG site inflammation: a useful diagnostic sign in incomplete Kawasaki disease. J Paediatr Child Health. 2008. 44:525–526.8. Sinha R, Balakumar T. BCG reactivation: a useful diagnostic tool even for incomplete Kawasaki disease. Arch Dis Child. 2005. 90:891.9. Hsu YH, Wang YH, Hsu WY, Lee YP. Kawasaki disease characterized by erythema and induration at the Bacillus Calmette-Guérin and purified protein derivative inoculation sites. Pediatr Infect Dis J. 1987. 6:576–578.10. de Zorzi A, Colan SD, Gauvreau K, Baker AL, Sundel RP, Newburger JW. Coronary artery dimensions may be misclassified as normal in Kawasaki disease. J Pediatr. 1998. 133:254–258.11. Olivieri L, Arling B, Friberg M, Sable C. Coronary artery Z score regression equations and calculators derived from a large heterogeneous population of children undergoing echocardiography. J Am Soc Echocardiogr. 2009. 22:159–164.12. Research Committee on Kawasaki Disease. Report of Subcommittee on Standardization of Diagnostic Criteria and Reporting of Coronary Artery Lesions in Kawasaki Disease. 1984. Tokyo: Ministry of Health and Welfare.13. Yu JJ, Jang WS, Ko HK, et al. Perivascular brightness of coronary arteries in Kawasaki disease. J Pediatr. 2011. 159:454–457.14. Sudo D, Monobe Y, Yashiro M, et al. Coronary artery lesions of incomplete Kawasaki disease: a nationwide survey in Japan. Eur J Pediatr. 2012. 171:651–656.15. Yun SH, Yang NR, Park SA. Associated symptoms of Kawasaki disease. Korean Circ J. 2011. 41:394–398.16. Barone SR, Pontrelli LR, Krilov LR. The differentiation of classic Kawasaki disease, atypical Kawasaki disease, and acute adenoviral infection: use of clinical features and a rapid direct fluorescent antigen test. Arch Pediatr Adolesc Med. 2000. 154:453–456.17. Yellen ES, Gauvreau K, Takahashi M, et al. Performance of 2004 American Heart Association recommendations for treatment of Kawasaki disease. Pediatrics. 2010. 125:e234–e241.18. Chang FY, Hwang B, Chen SJ, Lee PC, Meng CC, Lu JH. Characteristics of Kawasaki disease in infants younger than six months of age. Pediatr Infect Dis J. 2006. 25:241–244.19. Chuang CH, Hsiao MH, Chiu CH, Huang YC, Lin TY. Kawasaki disease in infants three months of age or younger. J Microbiol Immunol Infect. 2006. 39:387–391.20. Burns JC, Wiggins JW Jr, Toews WH, et al. Clinical spectrum of Kawasaki disease in infants younger than 6 months of age. J Pediatr. 1986. 109:759–763.21. Rowley AH, Gonzalez-Crussi F, Gidding SS, Duffy CE, Shulman ST. Incomplete Kawasaki disease with coronary artery involvement. J Pediatr. 1987. 110:409–413.22. Takayama J, Yanase Y, Kawasaki T. A study on erythematous change at the site of the BCG inoculation. Acta Paediatr Jpn. 1982. 86:567–572.23. Yanagawa H, Nakamura Y, Kawasaki T, Shigematsu I. Nationwide epidemic of Kawasaki disease in Japan during winter of 1985-86. Lancet. 1986. 2:1138–1139.24. Manlhiot C, Christie E, McCrindle BW, Rosenberg H, Chahal N, Yeung RS. Complete and incomplete Kawasaki disease: two sides of the same coin. Eur J Pediatr. 2012. 171:657–662.25. Perrin L, Letierce A, Guitton C, Tran TA, Lambert V, Koné-Paut I. Comparative study of complete versus incomplete Kawasaki disease in 59 pediatric patients. Joint Bone Spine. 2009. 76:481–485.26. Uehara R, Igarashi H, Yashiro M, Nakamura Y, Yanagawa H. Kawasaki disease patients with redness or crust formation at the Bacille Calmette-Guérin inoculation site. Pediatr Infect Dis J. 2010. 29:430–433.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Tuberculous Prostatic Abscess Following Intravesical Bacillus Calmette-Guerin Instillation
- Bacille Calmette-Guérin Osteomyelitis of the Distal Radius in a Toddler
- Early Detection of Kawasaki Disease in Infants
- Diagnosis and management of Kawasaki disease
- Clinical characteristics and serum N-terminal pro-brain natriuretic peptide as a diagnostic marker of Kawasaki disease in infants younger than 3 months of age
