J Cardiovasc Ultrasound.
2008 Dec;16(4):136-139. 10.4250/jcu.2008.16.4.136.
Loeffler's Endocarditis due to Idiopathic Hypereosinophilic Syndrome
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Dongsan Medical Center, Keimyung University, Daegu, Korea. khyungseop@dsmc.or.kr
- KMID: 1486395
- DOI: http://doi.org/10.4250/jcu.2008.16.4.136
Abstract
- Loeffler's endocarditis, a rare cardiac manifestation of hypereosinophilic syndrome (HES), is characterized by fibrous thickening of the endocardium of both ventricles, leading to apical obliteration and heart failure. We report a case of a 41-year-old male with slowly progressive right-sided heart failure symptoms. The complete blood count showed hypereosinophilia and the echocardiogram revealed that the both ventricles were filled with large amount of thrombus. His symptoms and typical echocardiographic findings markedly improved within several weeks after steroid and anticoagulation therapy.
MeSH Terms
Figure
-
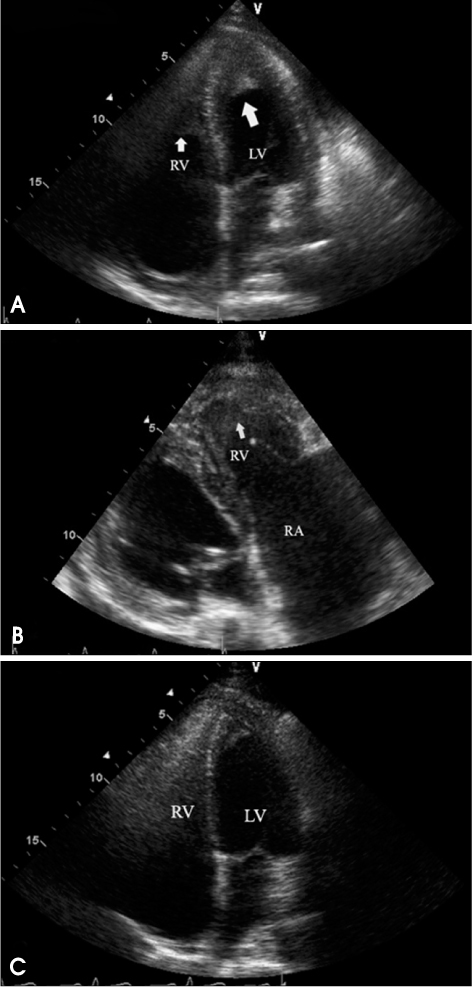
Fig. 1 Apical 4 chamber view of initial echocardiography showed apical homogeneous materials (arrows) suggestive of thrombi in the both ventricles (A). Right ventricular inflow view of initial echocardiography showed severe right atrial enlargement and large amount of thrombus filling in right ventricle (B). Apical 4 chamber view of follow up on the 15th hospital day showed marked resolution of thrombus at both ventricular apices (C).

Fig. 2 Computerized tomography of the chest showed apical obliterations of both ventricles by non-enhanced homogenous materials (arrow) consistent with the echocardiographic findings. The non-enhanced density material (arrowhead) was also noted in the enlarged right atrium.
Reference
-
1. Chusid MJ, Dale DC, West BC, Wolff SM. The hypereosinophilic syndrome; Analysis of fourteen cases with review of the literature. Medicine. 1975. 54:1–27.2. Tefferi A, Patnaik MM, Pardanani A. Eosinophilia: secondary, clonal and idiopathic. Br J Haematol. 2006. 133:468–492.
Article3. Corssmit EP, Trip MD, Durrer JD. Loeffler's endomyocarditis in the idiopathic hypereosinophilic syndrome. Cardiology. 1999. 91:272–276.
Article4. Gupta PN, Valiathan MS, Balakrishnan KG, kartha CC, Ghosh MK. Clinical course of endomyocardial fibrosis. Br Heart J. 1989. 62:450–454.
Article5. Chao BH, Cline-Parhamovich K, Grizzard JD, Smith TJ. Fatal Loeffler's endocarditis due to hypereosinophilic syndrome. Am J Hematol. 2007. 82:920–923.
Article6. Weller PF, Bubley GJ. The idiopathic hypereosinophilic syndrome. Blood. 1994. 83:2759–2779.
Article7. Lofiego C, Ferlito M, Rocchi G, Biagini E, Perugini E, Branzi A, Rapezzi C. Ventricular remodeling in Loeffler endocarditis: implications for therapeutic decision making. Eur J Heart Fail. 2005. 7:1023–1026.
Article8. Salanitri GC. Endomyocardial fibrosis and intracardiac thrombus occurring in idiopathic hypereosinophilic syndrome. Am J Roentgenol. 2005. 184:1432–1433.
Article9. Alter P, Maisch B. Endomyocardial fibrosis in Churg-Strauss syndrome assessed by cardiac magnetic resonance imaging. Int J Cardiol. 2006. 108:112–113.
Article10. Borer JS, Henry WL, Epstein SE. Echocardiographic observations in patients with systemic infiltrative disease involving the heart. Am J Cardiol. 1977. 39:184–188.
Article11. Parrillo JE, Borer JS, Henry WL, Wolff SM, Fauci AS. The cardiovascular manifestations of the hypereosinophilic syndrome. Prospective study of 26 patients, with review of the literature. Am J Med. 1979. 67:572–582.12. Klion AD. Approach to the treatment of hypereosinophilic syndrome. Immunol Allergy Clin North Am. 2007. 27:551–560.13. Lombardi C, Rusconi C, Faggiano P, Lanzani G, Campana C, Arbustini E. Successful reduction of endomyocardial fibrosis in a patient with idiopathic hypereosinophilic syndrome: A case report. Angiology. 1995. 46:345–351.
Article14. Cools J, DeAngelo DJ, Gotlib J, Stover EH, Legare RD, Cortes J, Kutok J, Clark J, Galinsky I, Griffin JD, Cross NC, Tefferi A, Malone J, Alam R, Schrier SL, Schmid J, Rose M, Vandenberghe P, Verhoef G, Boogaerts M, Wlodarska I, Kantarjian H, Marynen P, Coutre SE, Stone R, Gilliland DG. A tyrosine kinase created by fusion of the PDGFRA and FIP1L1 genes as a therapeutic target of imatinib in idiopathic hypereosinophilic syndrome. N Engl J Med. 2003. 348:1201–1214.
Article15. Butterfield JH. Treatment of hypereosinophilic syndromes with prednisone, hydroxyurea, and interferon. Immunol Allergy Clin North Am. 2007. 27:493–518.
Article16. Benezet-Mazuecos J, Marcos-Alberca P, Farré J, Orejas M, de la Fuente A, Prieto E. Images in cardiovascular medicine. Early differential resolution of right and left ventricular obliteration in Loeffler endocarditis after chemotherapy and anticoagulation. Circulation. 2006. 114:e635–e637.17. Benezet-Mazuecos J, de la Fuente A, Marcos-Alberca P, Farre J. Loeffler endocarditis: what have we learned? Am J Hematol. 2007. 82:861–862.
Article18. Morimoto S, Kubo N, Hiramitsu S, Uemura A, Ohtsuki M, Kato Y, Sugiura A, Miyagishima K, Mori N, Yoshida Y, Hishida H. Changes in the peripheral eosinophil count in patients with acute eosinophilic myocarditis. Heart Vessels. 2003. 18:193–196.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Loeffler's Endocarditis with Acute Obstruction of Common Iliac Artery
- A Case of Loeffler's Endocarditis Associated with Churg-Strauss Syndrome
- Early Stage Loeffler's Endocarditis Detected by Transthoracic Echocardiography
- Idiopathic Hypereosinophilic Syndrome Involving Thoracic Spine
- Loeffler Endocarditis: A Diagnosis Made with Cardiovascular Magnetic Resonance
