Nasal Reconstruction in the 21st Century: A Contemporary Review
- Affiliations
-
- 1Division of Facial Plastic and Reconstructive Surgery, Department of Otolaryngology-Head and Neck Surgery, University of Virginia Medical Center, Charlottesvill, USA. SPark@virginia.edu
- KMID: 1486028
- DOI: http://doi.org/10.3342/ceo.2008.1.1.1
Abstract
- Nasal restoration in the 21st century has reached a new milestone that has brought together centuries of experiences, lessons, errors, and rewards. The bar has been set and it is nothing less than a restoration of normal function and complete social acceptance. The aesthetic expectations of both minor and major nasal repair include symmetry, natural contour, excellent color and texture match, and a final product that remains inconspicuous to the casual observer. The major tenets that have been realized today include the wide application of the subunit principle, liberal and nonanatomic cartilage grafting (for form and function), and addressing each of the three layers of the nose independently. Anticipating resultant scars and vectors of tension during wound healing are the subtle nuances of nasal reconstruction that ensure a pleasing result. The robust nature of the forehead flap has proven to be a workhorse for major nasal resurfacing.
Keyword
MeSH Terms
Figure
-
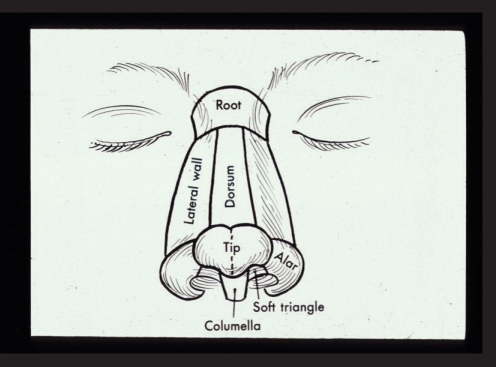
Fig. 1 Nasal aesthetic subunits defined.

Fig. 2 Aggressive thinning of forehead flap to subcutaneous plane.

Fig. 3 Large nasal defect following excision of skin cancer (A). Aesthetic units of nose and cheek (B). Aesthetic units completed with lateral wall batten graft for support (C). Forehead flap outlined (D). One year post-op, frontal (E) and close up oblique (F).
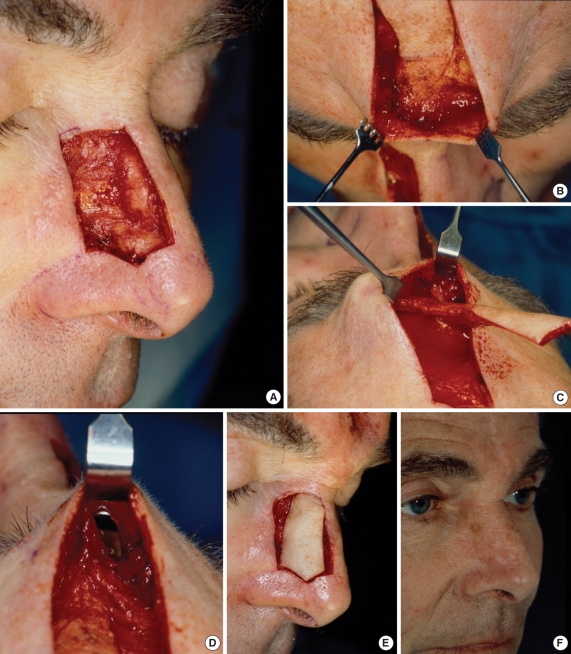
Fig. 4 Right sidewall defect, with aesthetic subunits completed (A). Glabellar skin lifted off pedicle (B). Forehead flap converted to an island flap (C). Tunnel created from forehead into nasal defect (D). Forehead flap passed under glabellar skin and filling nasal defect (E). One year result (F).

Fig. 5 Structural grafting to recreate framework of the lower 2/3's of the nose.

Fig. 6 Two nasal defects of sidewall and ala (A). Completion of aesthetic units and placement of large, "non-anatomic" conchal cartilage graft (B). One year post-op, oblique (C) and base views (D).

Fig. 7 Full thickness defect of left ala (A). Two layered composite graft harvested from ear (B). Composite graft inset and an interpolated melolabial flap designed (C). Flap in position with bolster dressing to hold composite graft against resurfacing flap (D). One year oblique (E) and base view (F).
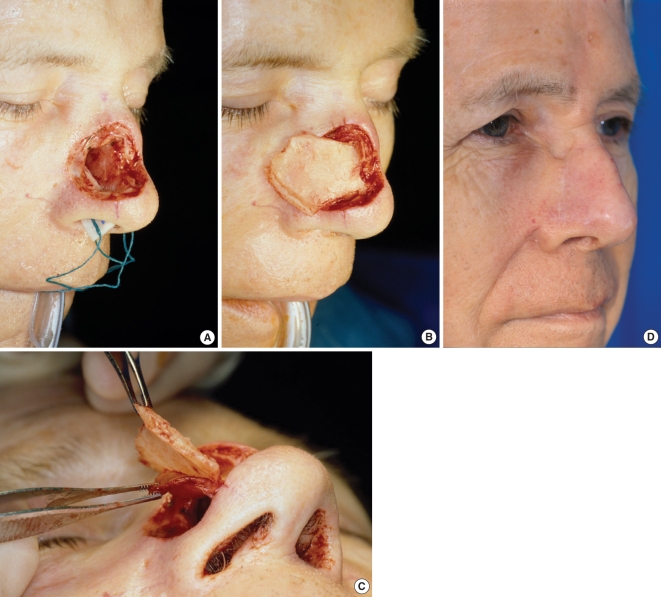
Fig. 8 Full thickness defect of the middle nasal vault (A). Composite septal flap, based on the dorsum, rotated outward (B). slight separation of septal cartilage and contralateral nasal septal mucosa, to allow cartilage to rest on bony piriform aperture and mucosa to be placed intranasally (C). Post operative oblique view (D).

Fig. 9 Subtotal, full-thickness nasal defect, frontal (A) and close-up oblique (B). Large ipsilateral septal mucosal flap for internal lining (C). Conchal cartilage for structure (D). Forehead flap (E). One year post operative frontal (F) and oblique views (G).
Cited by 1 articles
-
Tumor Control and Quality of Life in Skin Cancer Patients With Extensive Multilayered Nasal Defects
Michaela Plath, Hannah M. Thielen, Ingo Baumann, Karim Zaoui, Philippe A. Federspil
Clin Exp Otorhinolaryngol. 2020;13(2):164-172. doi: 10.21053/ceo.2019.00192.
Reference
-
1. Sushruta S. KK Bhishagratna. The Sushruta Samhita. 1907. Calcutta (India): Kaviraj Kunja Lal Bhishagratna.2. Larrabbee WF Jr, Sherris DA. Larrabee WF, Sherris DA, editors. Nose. Principles of facial reconstruction. 1995. Philadelphia (PA): Lippincott-Raven Publishers;p. 68–119.3. Burget GC, Menick FJ. The subunit principle in nasal reconstruction. Plast Reconstr Surg. 1985; 8. 76(2):239–247. PMID: 4023097.
Article4. Converse JM. New forehead flap for nasal reconstruction. Proc R Soc Med. 1942; 10. 35(12):811–812.5. Ugur MB, Savranlar A, Uzun L, Küçüker H, Cinar F. A reliable surface landmark for localizing supratrochlear artery: medial canthus. Otolaryngol Head Neck Surg. 2008; 2. 138(2):162–165. PMID: 18241709.
Article6. Quatela VC, Sherris DA, Rounds MF. Esthetic refinements in forehead flap nasal reconstruction. Arch Otolaryngol Head Neck Surg. 1995; 10. 121(10):1106–1113. PMID: 7546577.
Article7. Menick FJ. Baker SR, Swanson NA, editors. Reconstruction of the nose. Local flaps in facial reconstruction. 1995. St. Louis (MO): Mosby Year Book, Inc;p. 305–344.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Study for the Acoustic Characteristics of PB Word List according to Frequency
- Is Psychiatry Scientific? A Letter to a 21st Century Psychiatry Resident
- Medical history in the Korean History Textbook
- Current strategies for aesthetic soft tissue refinement in nasal reconstruction
- Neo-Elderly:The Way to Get Older Well
