Value of 3-Dimensional CT Virtual Anatomy Imaging in Complex Foreign Body Retrieval from Soft Tissues
- Affiliations
-
- 1Department of Radiology, Shanghai Eighth People's Hospital, Shanghai 200235, China. woothingyang2008@126.com
- 2Department of General Surgery, Shanghai Eighth People's Hospital, Shanghai 200235, China.
- KMID: 1482786
- DOI: http://doi.org/10.3348/kjr.2013.14.2.269
Abstract
OBJECTIVE
To investigate the value of 3-dimensional (3D) CT virtual anatomy imaging (VAI) in the complex foreign body (FB) retrieval of the soft tissues.
MATERIALS AND METHODS
Four hundred and seventy-five patients with radiopaque FB(s) diagnosed by radiograph underwent contrast-enhanced 3D CT examination. VAI was reconstructed by volume-rendering opacity software, by sliding down the lowest threshold from -600 to 100 HU. The imaging was grouped into three groups: A (axial and multi-planar reformation [MPR] images), B (standard 3D imaging with axial and MPR images), and C (VAI with axial and MPR images). They were analyzed to reveal the type, size, number, location, complications, and the interventional removability of the object, with the comparisons in the management and clinical outcomes on the patient follow-up studies. The data were subjected to chi-square tests, with p value < 0.05 indicating significant statistical difference.
RESULTS
The FB shape, size, number, site distribution and vessels around FB, as well as the FB-associated vascular complications and the FB interventional removability were assessed more accurately in Group C than in Group B or Group A (p < 0.005). There was no significant difference in disclosing the type and depth of the FB among the three groups (p > 0.75). On the basis of the 3D CT, especially the enhanced 3D CT VAI, the followings were processed: the recommendation of interventional removal in 286 (60.47%) and non-intervention in 187 (39.53%) of the 473 patients with soft-tissue FB(s); in 352 (56.50%) of the 623 radiopaque FBs patients, 258 (54.55%) patients accurately detected on 3D CT and the successful removal by intervention (343 FBs) or surgery (9 FBs) without any sequela; and 215 (45.45%) patients with 271 FBs lost in the follow-up, with their departure from the hospital.
CONCLUSION
The 3D CT, especially 3D enhanced CT VAI, has great incremental value in further diagnosis and management of complex FB extraction from soft tissues.
Keyword
MeSH Terms
-
Adolescent
Adult
Aged
Contrast Media/diagnostic use
Female
Foreign Bodies/*radiography/surgery
Humans
*Imaging, Three-Dimensional
Iohexol/diagnostic use
Male
Middle Aged
Radiographic Image Interpretation, Computer-Assisted
Tomography, X-Ray Computed/*methods
Treatment Outcome
User-Computer Interface
Contrast Media
Iohexol
Figure
-
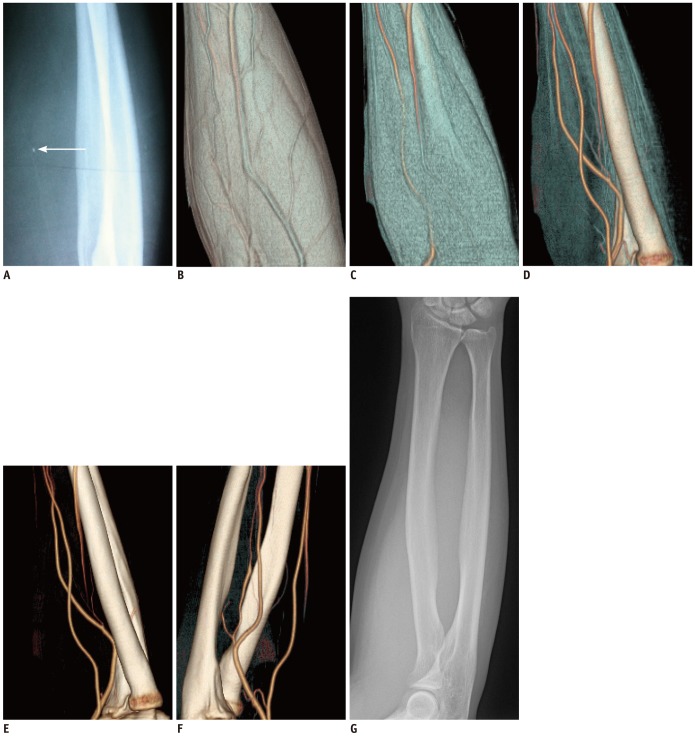
Fig. 1 False positive of soft-tissue FB detected by radiograph.FB (arrow, 2 mm in diameter) in right forearm disappears 21 days after being diagnosed by radiograph (A) in 52-year-old male patient. 3D CT VAI shows no FB from superficial (B), muscles (C), tendons (D) to deep arteries and bones (E), and their rotating image (F). Subsequent radiograph (G) and follow up prove CT finds. FB = foreign body, 3D = 3-dimensional, VAI = virtual anatomy imaging
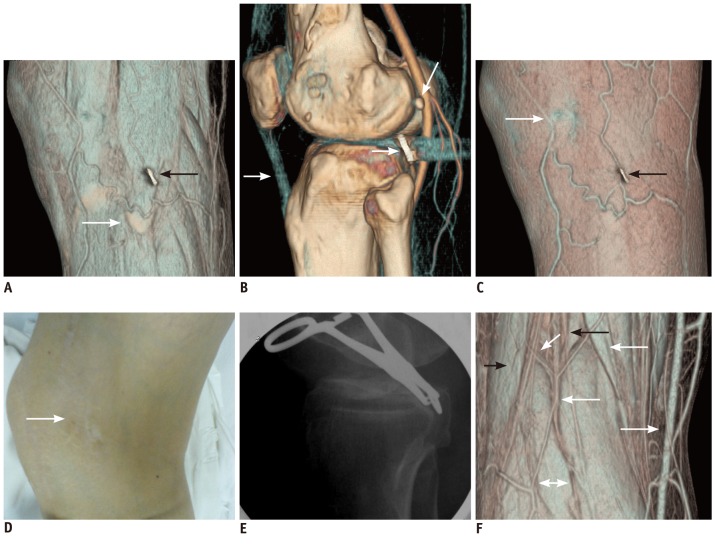
Fig. 2 Screw cap (10 mm in diameter and 1 mm thickness) fell off and remained in soft tissues around knee for 8 years, after internal fixation of left knee, in 50-year-old female patient.Muscle view of VAI (A) clearly shows relationship of FB with fibular head (dovetail arrow) and superficial veins around knee, and damage to biceps femoris tendon (black arrow). Diameter, thickness of FB, and its minimal interval to popliteal artery and fibular head are visualized accurately on arterial view (B). Patellar ligament (white arrow) is clearly visible. Differentiation of sesamoidea (curving arrow) and FB (dovetail arrow) is noted differently here. Imprint of FB (black arrow), adjacent subcutaneous veins, and surgical scar (dashed arrow) are displayed clearly on superficial view (C) in accordance with actual conditions (D). Using Allis' forceps to clamp screw cap in its central hole, FB was removed successfully under guiding fluoroscopy (E) without any complications. Muscle view of popliteal space (F) 3D shows normal structures of biceps femoris tendon (black arrow), semitendinosus muscle (white arrow), gastrocnemius (left-right arrow), popliteal vein (dashed arrow), small saphenous vein (white dovetail arrow), common peroneal nerve (curving arrow), and tibial nerve (black dovetail arrow). FB = foreign body, 3D = 3-dimensional, VAI = virtual anatomy imaging
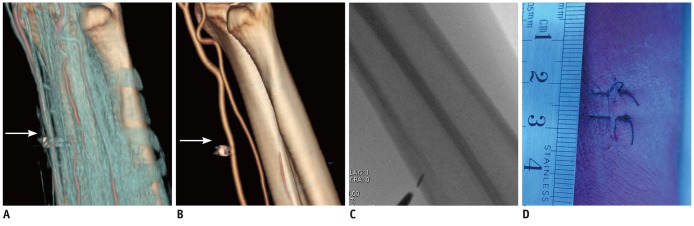
Fig. 3 62-years-old male patient with soft-tissue injury in right forearm by metallic FB (arrow), adjacent to radial artery.Key structures, especially vessels adjacent to FB, are situated only in one side and no vital vessels and other important structures are observed in its superficial side on tendon view image (A) and arterial view image (B) of VAI. Open incision is thus recommended, with fluoroscopic guiding, precise localization of object (C), and local anesthesia, for direct exposure of FB and its retrieval. Procedure left 2 cm suture in local skin (D); FB was removed successfully, and patient recovered without any sequelae. FB = foreign body, VAI = virtual anatomy imaging
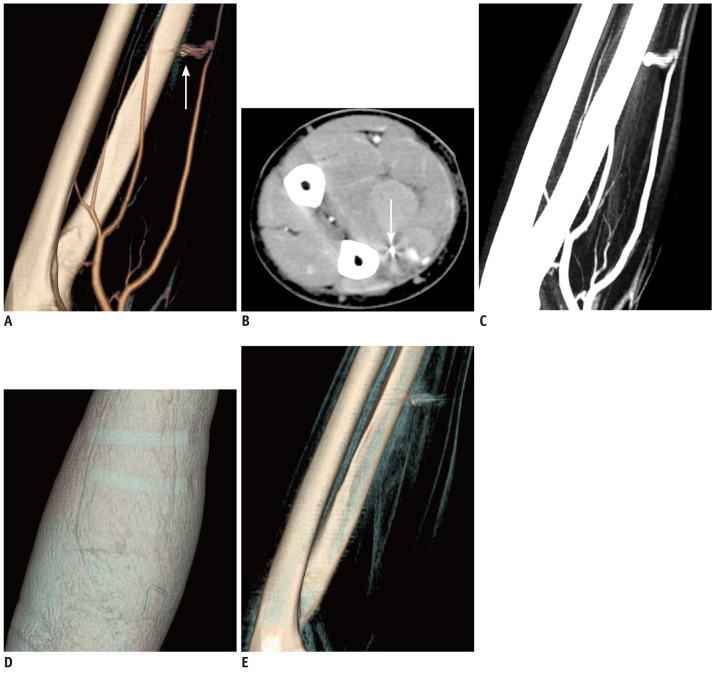
Fig. 4 On outward apearance and physical examination only, FB-associated pseudoaneurysm can not be found.45-year-old male patient with small steel patch (arrow) in left forearm and FB-associated vascular complications of irregular pseudoaneurysm and arteriospasm of distal radial artery, shown on VAI images of arterial view (A), which is contraindication of FB interventional removal. Pseudoaneurysm is not shown on axial contrast-enhanced CT images (B), and FB cannot be distinguished from pseudoaneursym on routine CT, even 3D MIP images (C). From appearance only, including skin view images (D) of VAI, FB, vascular injuring complications, and potential risks of retained FB, and in particular removal risks, cannot be discovered. On non-enhanced VAI (E), arteries, deep veins, and traumatic pseudoaneurysm shown on contrast-enhanced VAI (A, C) were not visualized clearly. FB = foreign body, VAI = virtual anatomy imaging, MIP = maximum intensity projection
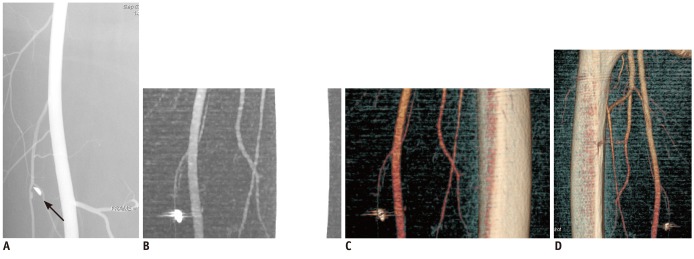
Fig. 5 False negative of FB-associated traumatic pseudoaneurysm on 3D CT VAI.40-years-old male patient with metallic soft-tissue FB in his left thigh and small FB-associated traumatic pseudoaneurysm (arrow, 2 × 3 × 1 mm in size) shown in FB adjacent branch femoral artery on angiograms (A). 3D MIP (B) and VAI with rotation and threshold adjusting (C, D) show no pseudoaneurysm near FB arteries. Sharp shape of FB is shown as obtuse on 3D CT. FB = foreign body, 3D = 3-dimensional, VAI = virtual anatomy imaging, MIP = maximum intensity projection
Reference
-
1. Callegari L, Leonardi A, Bini A, Sabato C, Nicotera P, Spano' E, et al. Ultrasound-guided removal of foreign bodies: personal experience. Eur Radiol. 2009; 19:1273–1279. PMID: 19153745.
Article2. Park TH, Seo SW, Kim JK, Chang CH. Clinical outcome in a series of 173 cases of foreign body granuloma: improved outcomes with a novel surgical technique. J Plast Reconstr Aesthet Surg. 2012; 65:29–34. PMID: 21885359.
Article3. Ando A, Hatori M, Hagiwara Y, Isefuku S, Itoi E. Imaging features of foreign body granuloma in the lower extremities mimicking a soft tissue neoplasm. Ups J Med Sci. 2009; 114:46–51. PMID: 19242872.
Article4. Nocturne G, Sellam J, Miquel A, M'Bappé P, Berenbaum F. Is sarcoma a complication of arterial femoro-popliteal bypass? Joint Bone Spine. 2010; 77:358–360. PMID: 20471894.
Article5. Hunter TB, Taljanovic MS. Foreign bodies. Radiographics. 2003; 23:731–757. PMID: 12740473.
Article6. Young AS, Shiels WE 2nd, Murakami JW, Coley BD, Hogan MJ. Self-embedding behavior: radiologic management of self-inserted soft-tissue foreign bodies. Radiology. 2010; 257:233–239. PMID: 20823372.
Article7. Lammers RL. Soft tissue foreign bodies. Ann Emerg Med. 1988; 17:1336–1347. PMID: 3057951.
Article8. Lammers RL, Magill T. Detection and management of foreign bodies in soft tissue. Emerg Med Clin North Am. 1992; 10:767–781. PMID: 1425403.
Article9. Bakshi J, Verma RK, Karuppiah S. Migratory foreign body of neck in a battered baby: a case report. Int J Pediatr Otorhinolaryngol. 2009; 73:1814–1816. PMID: 19879659.
Article10. Croy T. Metallic foreign body in a patient with knee pain. J Orthop Sports Phys Ther. 2011; 41:696. PMID: 21885912.
Article11. Hecht S, Adams WH, Narak J, Thomas WB. Magnetic resonance imaging susceptibility artifacts due to metallic foreign bodies. Vet Radiol Ultrasound. 2011; 52:409–414. PMID: 21382122.
Article12. Kiliç A, Avcu S, Tekïn S, Gül A, Cïnal A, Yasar T. MRI-Induced Migration of Retained Metallic Foreign Body in the Eye. Ophthalmic Surg Lasers Imaging. 2010; 1–3.
Article13. Sun Z. 3D multislice CT angiography in post-aortic stent grafting: a pictorial essay. Korean J Radiol. 2006; 7:205–211. PMID: 16969051.
Article14. Meurer WJ. Radial artery pseudoaneurysm caused by occult retained glass from a hand laceration. Pediatr Emerg Care. 2009; 25:255–257. PMID: 19369839.
Article15. Tao K, Xu S, Liu XY, Liang JL, Qiu T, Tan JN, et al. Small metal soft tissue foreign body extraction by using 3D CT guidance: a reliable method. Eur J Radiol. 2012; 81:3339–3343. PMID: 22321905.
Article16. Nemsadze G, Urushadze O. The role of multislice spiral computed tomography in the diagnosis and management of acute facial trauma in patients with multiple injuries. Georgian Med News. 2011; 11:36–42. PMID: 22201078.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Virtual Endoscopy of Impacted Foreign Bodies in Tracheal and Esophageal Model
- The Utility of Three-dimensional CT in Orbital Diseases
- Percutaneous Retrieval of a Migrated Surgical Drainage Tube in the Chest Wall with the Nitinol Goose Neck Snare
- Usefulness of Two-dimensioanl CT & Three-dimensional CT in Blow-out Fracture
- MDCT Application of Thoracic Imaging
