Nonunion with a Bony Defect of the Humerus: Treatment by Shortening
- Affiliations
-
- 1Department of Orthopaedic Surgery, Yong-San Hospital, Chung-Ang University College of Medicine, Seoul, Korea. sooykang@hitel.net
- KMID: 1480963
- DOI: http://doi.org/10.12671/jkfs.2008.21.1.45
Abstract
-
PURPOSE: To evaluate clinical results and advantage of interposition and shortening technique for the treatment of the humeral nonunion with bone defect.
MATERIALS AND METHODS
Eight patients with the humeral nonunion with bone defect underwent interposition of fragments and shortening had been followed-up for more than one year (mean 70 months, 16~156). There were 4 men and 4 women with a mean age of 60.5 years (range, 48 to 75 years). There included 3 proximal, 3 diaphysis and 2 distal metaphysis according to the site, mean size of the bone defect was 3.3 cm (2~5). The time to union, discrepancy of upper extremity, functional results, cosmetic satisfaction and postoperative complications were assessed.
RESULTS
All patients achieved to bone union, average union time was 10.2 weeks (range 8~14). Average limb discrepancy was 2.3 cm. All had improvement in shoulder and elbow motion after operation. Seven patients were satisfied with the cosmetic result and none had functional deficit due to limb discrepancy.
CONCLUSION
Treatment by Interposition of fragments and shortening in the intractable nonunion of humerus with a bony defect can achieve not only good functional result, shortened bone union time and improved in shoulder and elbow motion.
Keyword
MeSH Terms
Figure
-

Fig. 1 Schematic illustration of the shortening and interposition technique.

Fig. 2 50-year-old woman presented with pain and motion limitation of left elbow. (A) Preoperative radiograph shows nonunion with 5 cm bone defect of supracondylar area of the humerus. (B) Postoperative radiograph shows interposition of the distal fragment to the proximal fragment and external fixation. (C) 12 months after operation, bone union was achieved. (D) The arc of ulnohumeral motion was checked 20 to 110 degree and limb discrepancy was checked 4.5 cm.
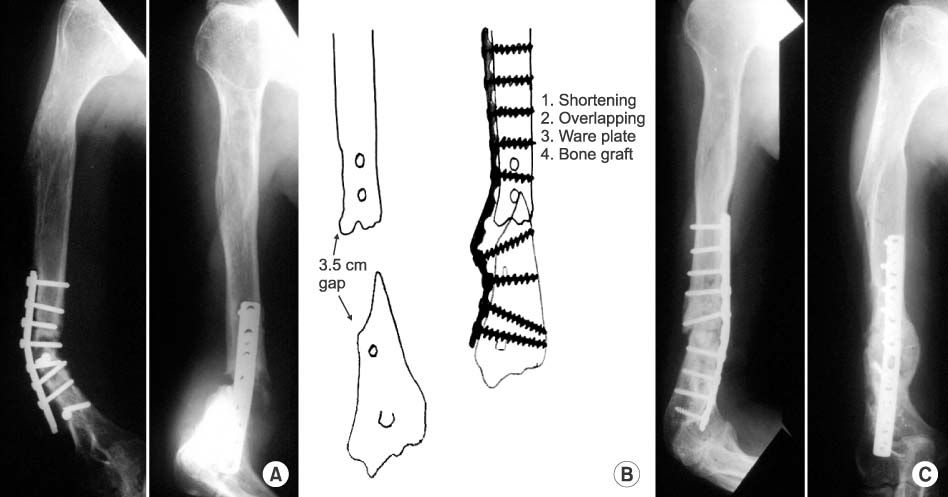
Fig. 3 75 year-old male presented with pain and weakness of right arm after opearative fixation of a fracture of the distal shaft of the humerus. (A) Anteroposterior radiograph demonstrating nonunion with bony defect and screw loosening. (B) The preoperative plan. (C) 2 months after a wave plate and autogenous bone graft had been applied, bone union was achieved and the limb discrepancy wad checked 2 cm.
Reference
-
1. Beredjiklian PK, Hotchkiss RN, Athanasian EA, Ramsey ML, Katz MA. Recalcitrant nonunion of the distal humerus: treatment with free vascularized bone grafting. Clin Orthop Relat Res. 2005; 435:134–139.2. Foster RJ, Dixon GL Jr, Bach AW, Appleyard RW, Green TM. Internal fixation of fractures and non-unions of the humeral shaft. Indications and results in a multi-center study. J Bone Joint Surg Am. 1985; 67:857–864.
Article3. Hosny GA. Unilateral humeral lengthening in children and adolescents. J Pediatr Orthop B. 2005; 14:439–443.
Article4. Jupiter JB, von Deck M. Ununited humeral diaphyses. J Shoulder Elbow Surg. 1998; 7:644–653.
Article5. Muller M, Allgower M, Schneider R, Willenergger H. Manual of internal fixation. 3rd ed. Berlin etc: Springer;1991. p. 738.6. Perren SM. The concept of biological plating using the limited contact-dynamic compression plate (LC-DCP). Scientific background, design and application. Injury. 1991; 22:Suppl 1. 1–41.
Article7. Pullen C, Manzotti A, Catagni MA, Guerreschi F. Treatment of post-traumatic humeral diaphyseal nonunion with bone loss. J Shoulder Elbow Surg. 2003; 12:436–441.
Article8. Ring D, Allende C, Jafarnia K, Allende BT, Jupiter JB. Ununited diaphyseal forearm fractures with segmental defects: plate fixation and autogenous cancellous bonegrafting. J Bone Joint Surg Am. 2004; 86:2440–2445.
Article9. Ring D, Jupiter JB, Quintero J, Sanders RA, Marti RK. Atrophic ununited diaphyseal fractures of the humerus with a bony defect: treatment by wave-plate osteosynthesis. J Bone Joint Surg Br. 2000; 82:867–871.10. Sarmiento A, Zagorski JB, Zych GA, Latta LL, Capps CA. Functional bracing for the treatment of fractures of the humeral diaphysis. J Bone Joint Surg Am. 2000; 82:478–486.
Article11. Van Houwelingen AP, McKee MD. Treatment of osteopenic humeral shaft nonunion with compression plating, humeral cortical allograft struts, and bone grafting. J Orthop Trauma. 2005; 19:36–42.
Article12. Zagorski JB, Latta LL, Zych GA, Finnieston AR. Diaphyseal fractures of the humerus. Treatment with prefabricated braces. J Bone Joint Surg Am. 1988; 70:607–610.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Compression Plate Fixation with Autogenous Bone Graft for Humerus Shaft Nonunion
- The IliBarov Technique in the Treatment of Nonunions of Long Bone
- Nonunion of the Fractures of the Distal Humerus: A Report of 6 Cases
- Treatment of nonunion of proximal tibia: Treatment using external fixator
- The Clinical Results in Compression Plate Fixation with Autogenous Cancellous Bone Graft for Humerus Diaphyseal Nonunion
