Graves' Disease Accompanied by Pheochromocytoma: Report of a Case
- Affiliations
-
- 1Division of Endocrinology, Chosun University Hospital, Korea.
- KMID: 1468508
- DOI: http://doi.org/10.3803/jkes.2009.24.2.126
Abstract
- We present here a rare case of Graves' disease accompanied by pheochromocytoma, and the patient showed normal urine and serum levels of catecholamines and their metabolites. A 45-year-old woman was referred to our hospital for the evaluation of a right adrenal incidentaloma that was detected by chest computed tomography. She had been diagnosed with Graves' disease 1 month previously. She had no symptoms of pheochromocytoma such as hypertension or a history of hypertension attack. Two consecutive 24-hour urine samples were sent to the lab for measurement of the catecholamines, and both samples showed normal levels of metanephrine and vanillylmandelic acid (VMA). After right adrenalectomy was performed, the final pathological diagnosis was adrenal pheochromocytoma. This case suggests that the onset of Graves' disease may be associated with excess catecholamine secreted by a pheochromocytoma. In addition, although the conventional method for detecting pheochromocytoma is to identify an increase of the urine catecholamines, physicians should be aware of the possibility of false negativity on this test.
Keyword
MeSH Terms
Figure
-
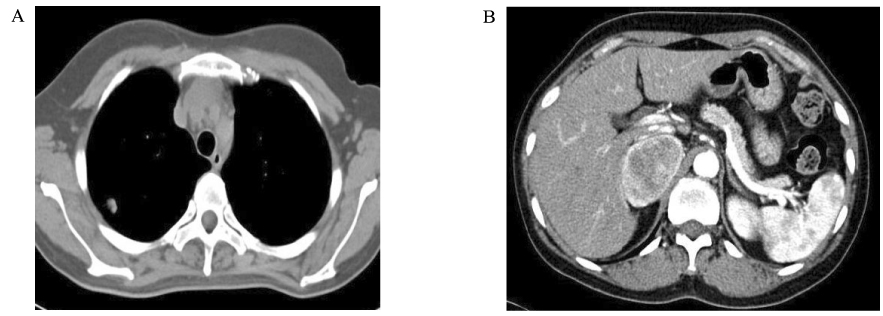
Fig. 1 Chest computed tomography (CT) and Abdominal CT. A. Chest CT showed a 1.2 cm unenhanced SPN in the right upper lobe. B. Abdominal CT revealed a 4.8 × 3.6 cm heterogenously enhanced mass in the right adrenal gland.

Fig. 2 Gross appearance after right adrenalectomy. Resected adrenal gland showed encapsulated ovoid mass and diffuse areas of hemorrhages.
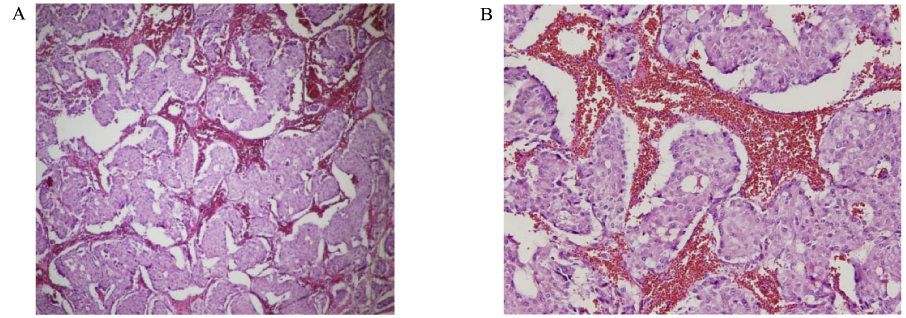
Fig. 3 Microscopic features of pheochromocytoma. Nests of tumor cells ("Zellballen") are separated by thin connective tissue stroma, containing abundant thin walled blood vessels. The tumor cells have oval nuclei and abundant granular cytoplasm. (A) H&E ×40 (B) H&E ×200.
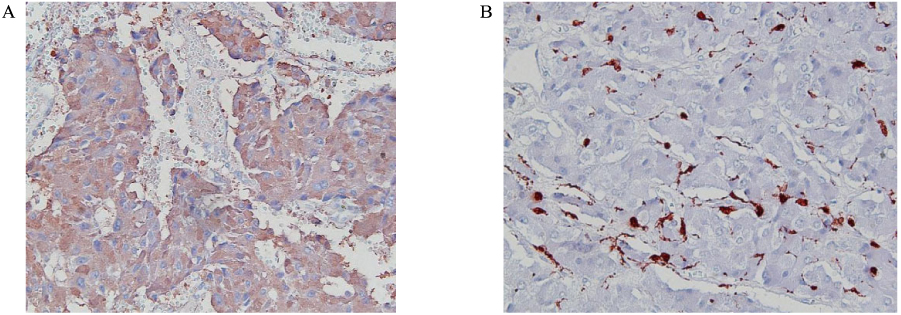
Fig. 4 Immunohistochemistry stain of pheochromocytoma. There is positive for chromogranin (A) and S-100 protein (B).
Reference
-
1. Weetman AP. Graves' disease. N Engl J Med. 2000. 343:1236–1248.2. Chiovato L, Pinchera A. Stressful life events and Graves' disease. Eur J Endocrinol. 1996. 134:680–682.3. Liggett SB, Shan SD, Cryer PE. Increased fat and skeletal muscle beta-adrenergic receptors but unaltered metabolic and hemodynamic sensitivity to epinephrine in vivo in experimental human thyrotoxicosis. J Clin Invest. 1989. 83:803–809.4. Toccafondi RS, Brandi ML, Rotella CM, Zonefrati R. Studies of catecholamine effect on cyclic AMP in human cultured thyroid cells: their interaction with thyrotrophin receptor. Acta Endocrinol (Copenh). 1983. 102:62–67.5. Martin A, Nakashima M, Zhou A, Aronson D, Werner AJ, Davies TF. Detection of major T cell epitopes on human thyroid stimulating hormone receptor by overriding immune heterogenecity in patients with Graves' disease. J Clin Endocrinol Metab. 1997. 82:3361–3366.6. Tanwani LK, Lohano V, Ewart R, Broadstone VL, Mokshagundam SP. Myasthenia gravis in conjunction with Graves' disease: a diagnostic challenge. Endocr Pract. 2001. 7:275–278.7. Biro E, Szekanecz Z, Czirjak L, Danko K, Kiss E, Szabo NA, Szucs G, Zeher M, Bodolay E, Szegedi G, Bako G. Association of systemic and thyroid autoimmune diseases. Clin Rheumatol. 2006. 25:240–245.8. Nagai T, Imamura M, Kamiya Y, Mori M. Graves' disease accompanied by anti-myeloperoxidase antibody-related nephropathy and autoimmune hepatitis. Intern Med. 2004. 43:516–520.9. Akinyemi OO, Lawani J. Anaesthetic management of pheochromocytoma in the presence of hyperthyroidism. East Afr Med J. 1980. 57:795–798.10. Braverman LE, Sullivan RM. Another polyendocrine disorder: pheochromocytoma and diffuse toxic goiter. Johns Hopkins Med J. 1969. 125:331–335.11. Shmurun RI. Extra-adrenal pheochromocytoma associated with bilateral diffuse-nodular hyperplasia of the adrenal cortex and micro-macrofollicular goiter. Arkh Patol. 1976. 38:57–60.12. Snow MH, Burton P. A case of associated thyrotoxicosis and pheochromocytoma. A diagnostic problem. Postgrad Med J. 1976. 52:288–291.13. Paschke R, Enger I, Harsch I, Usadel KH. Relapse of Graves' disease following development of a pheochromocytoma. Thyroid. 1992. 2:203–206.14. Abe M, Mori K, Nagai K, Ito S. Relapse of Graves' disease in a patient with pheochromocytoma. Endocr J. 2003. 50:767–770.15. Kim HS, Joo HJ, Choi YS, Kim ES, Park SY, Lee YJ, Kim HY, Seo JA, Kim SG, Choi DS. A case of Graves' disease with pheochromocytoma. J Korean Endocr Soc. 2007. 22:465–469.16. Lenders JW, Eisenhofer G, Mannelli M, Pacak K. Phaeochromocytoma. Lancet. 2005. 366:665–675.17. Ahren B. Effects of α-adrenoceptor agonists and antagonists on thyroid hormone secretion. Acta Endocrinol (Copenh). 1985. 108:184–191.18. Di Paola R, Menzaghi C, De Filippis V, Corda D, Di Cerbo A. Cyclooxygenase-dependent thyroid cell proliferation induced by immunoglobulins from patients with Graves' disease. J Clin Endocrinol Metab. 1997. 82:670–673.19. Yamada T, Sato A, Komiya I, Nishimori T, Ito Y, Terao A, Eto S, Tanaka Y. An elevation of serum immunoglobulin E provides a new aspect of hyperthyroid Graves' disease. J Clin Endocrinol Metab. 2000. 85:2775–2778.20. Stein PP, Black HR. A simplified diagnostic approach to pheochromocytoma. A review of the literature and report of one institution's experience. Medicine (Baltimore). 1991. 70:46–66.21. Lenders JW, Pacak K, Walther MM, Linehan WM, Mannelli M, Friberg P, Keiser HR, Goldstein DS, Eisenhofer G. Biochemical diagnosis of pheochromocytoma: which test is best? JAMA. 2002. 287:1427–1434.22. Gerlo EA, Sevens C. Urinary and plasma catecholamines and urinary catecholamine metabolites in pheochromocytoma: diagnostic value in 19 cases. Clin Chem. 1994. 40:250–256.23. Stewart MF, Reed P, Weinkove C, Moriarty KJ, Ralston AJ. Biochemical diagnosis of pheochromocytoma: two instructive case reports. J Clin Pathol. 1993. 46:280–282.24. Ozkaya M, Yuzbasioglu MF, Bulbuloglu E, Bakaris S, Oksuz H, Gisi K, Onder A. Incidental pheochromocytoma presenting with sublaboratory findings in asymptomatic surrenal masses: a case report. Cases J. 2008. 1:10.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Graves' Disease with Pheochromocytoma
- A Case of Cystic Pheochromocytoma
- A Case of Malignant Pheochromocytoma
- A Case of Methimazole-induced Agranulocytosis and Kikuchi's Disease in a Patient with Graves' Disease
- Persistent Hypokalemic Paralysis in a Patient with Graves’ Disease and Gitelman Syndrome
