Multilevel Duodenal Injury after Blunt Trauma
- Affiliations
-
- 1Department of Surgery, College of Medicine, Hallym University, Chuncheon, Korea. byryu@hallym.or.kr
- KMID: 1464888
- DOI: http://doi.org/10.4174/jkss.2009.77.4.282
Abstract
- Duodenal trauma is an uncommon injury associated with significant mortality and morbidity. Upper gastrointestinal radiological studies and computed tomography may lead to the diagnosis of blunt duodenal trauma. Exploratory laparotomy remains as the ultimate diagnostic test if a high suspicion of duodenal injury continues even in the face of absent or equivocal radiographic signs. The majority of duodenal injuries may be managed by simple repair of the injured site. More complicated injuries require more sophisticated techniques. Here, we report a case of multilevel blunt duodenal injury successfully managed with duodenal diverticulization, Roux-en-Y gastrojejunostomy and catheter duodenostomy.
Figure
-
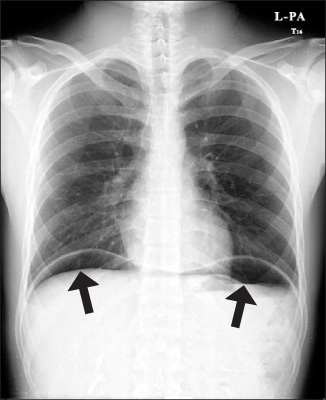
Fig. 1 Thoracic radiograph shows pneumoperitoneum in the bilateral subphrenic areas (arrows).
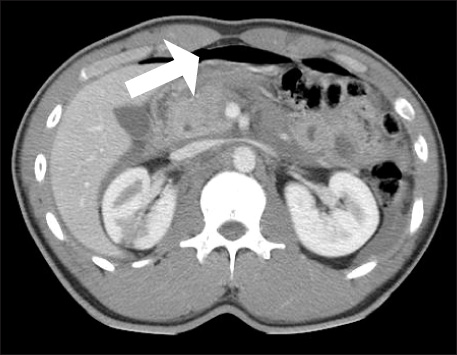
Fig. 2 Abdomen computed tomography scan shows the findings of pneumoperitoneum (arrows).
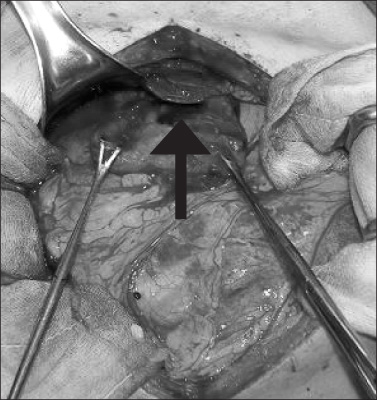
Fig. 3 Duodenal disruption (75% of the circumference, grade 3) is present on the first part of duodenum (arrow).
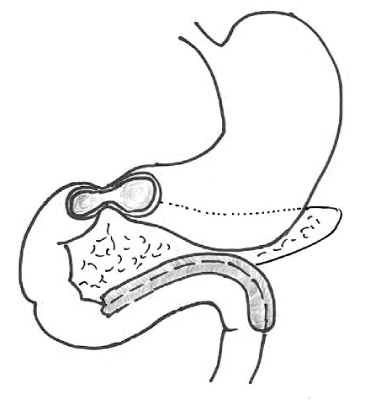
Fig. 4 Duodenal perforation with multiple injury. Duodenal disruption (75% of the circumference, grade 3) is present on the first part of duodenum. The serosa of the third and fourth part of duodenum is detached from pancreas and the segments devasculized.
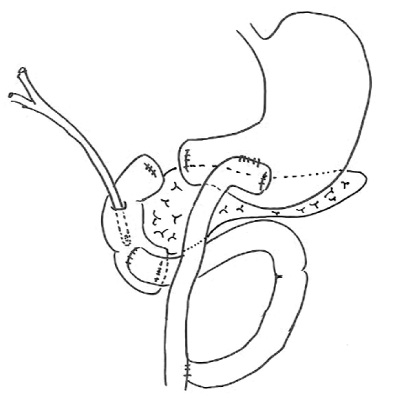
Fig. 5 Operative management. Duodenal diverticulization is performed with the duodenal resection of the 1st, 3rd, 4th parts. Side to side Roux-en-Y gastrojejunostomy was performed and side-to-side duodenojejunostomy using afferent jejunal loop was performed. Catheter duodenostomy using foley catheter was performed.
Reference
-
1. Carrillo EH, Richardson JD, Miller FB. Evolution in the management of duodenal injuries. J Trauma. 1996. 40:1037–1045.2. Lucas CE, Ledgerwood AM. Factors influencing outcome after blunt duodenal injury. J Trauma. 1975. 15:839–846.3. Moore EE, Cogbill TH, Malangoni MA, Jurkovich GJ, Champion HR, Gennarelli TA, et al. Organ injury scaling, II: pancreas, duodenum, small bowel, colon, and rectum. J Trauma. 1990. 30:1427–1429.4. Jurkovich GJ, Bulger EM. Moore EE, Feliciano DV, Mattox KL, editors. Duodenum and pancreas. Trauma. 2004. 5th ed. New York: McGraw-Hill;709–734.5. Huerta S, Bui T, Porral D, Lush S, Cinat M. Predictors of morbidity and mortality in patients with traumatic duodenal injuries. Am Surg. 2005. 71:763–767.6. Snyder WH 3rd, Weigelt JA, Watkins WL, Bietz DS. The surgical management of duodenal trauma. Precepts based on a review of 247 cases. Arch Surg. 1980. 115:422–429.7. Lucas CE, Dulchavsky SA, Ledgerwood AM. Hurst JM, editor. Pancreaticoduodenal injury. Common Problems in Trauma. 1987. Chicago: Year Book Medical Publishers;204–212.8. Yutan E, Waitches GM, Karmy-Jones R. Blunt duodenal rupture: complementary roles of sonography and CT. AJR Am J Roentgenol. 2000. 175:1600.9. Miller LA, Shanmuganathan K. Multidetector CT evaluation of abdominal trauma. Radiol Clin North Am. 2005. 43:1079–1095.10. Lopez PP, Benjamin R, Cockburn M, Amortegui JD, Schulman CI, Soffer D, et al. Recent trends in the management of combined pancreatoduodenal injuries. Am Surg. 2005. 71:847–852.11. Asensio JA, Petrone P, Roldan G, Kuncir E, Demetriades D. Pancreaticoduodenectomy: a rare procedure for the management of complex pancreaticoduodenal injuries. J Am Coll Surg. 2003. 197:937–942.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Duodenal Injury after Blunt Abdominal Trauma: Report of Two Cases
- Isolated Duodenal Injury following Blunt Abdominal Trauma
- Delayed manifestation of Isolated Intramural Hematoma of the duodenum resulting from Blunt abdominal Trauma
- Caval Injury due to Blunt Trauma: A Report of Two cases
- Very large haematoma following the nonoperative management of a blunt splenic injury in a patient with preexisting liver cirrhosis: a case report
