J Korean Fract Soc.
2010 Oct;23(4):386-390. 10.12671/jkfs.2010.23.4.386.
False Negative Bone Scan in 56-year Old Man with L2 Compression Fracture Performed 78 Hours after Trauma: A Case Report
- Affiliations
-
- 1Department of Orthopedic Surgery, Seoul Paik Hospital, Inje University College of Medicine, Seoul, Korea. hd1404@hanafos.com
- KMID: 1461497
- DOI: http://doi.org/10.12671/jkfs.2010.23.4.386
Abstract
- It is very rare that the bone scan after 72 hours from the trauma doesn't exhibit the increased radio-nuclide uptake in the patient with fracture. The purpose of this study is to report the case that indicate the false negative finding in the bone scan performed after 78 hours from the trauma in the 56-year-old man with L2 compression fracture, including a review of the relevant literatures.
MeSH Terms
Figure
-
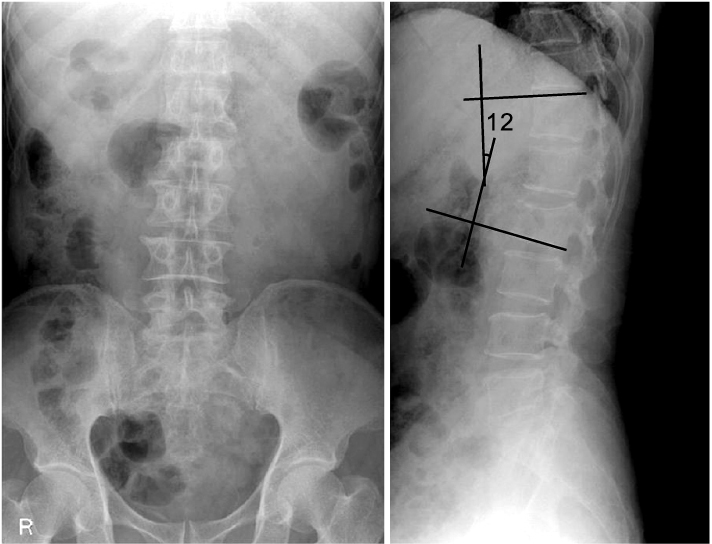
Fig. 1 Radiographs show anterior compression and kyphosis of L2 vertebral body in AP and lateral view.
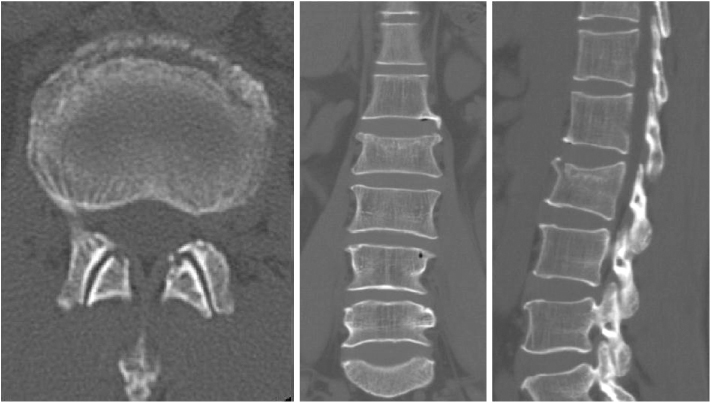
Fig. 2 CT scan shows compression of L2 vertebral body.
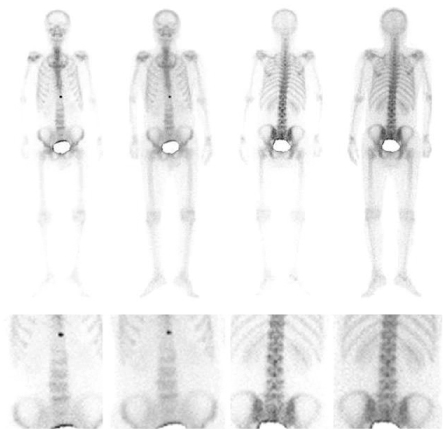
Fig. 3 Bone scan performed at 78 hours of post-trauma shows no abnormal uptake in L2 vertebra.

Fig. 4 MRI performed at 2 months after trauma shows signals indicating recently developed compression fracture of L2 vertebra.
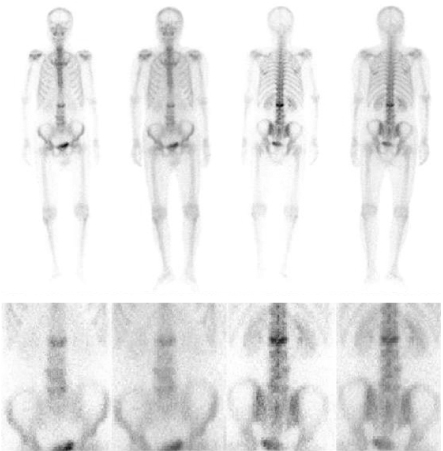
Fig. 5 Bone scan performed at 2 months after trauma shows increased uptake in L2 vertebra.
Reference
-
1. Jung JH, Kim JK, Jin W, et al. The value of radionuclide imaging as a screening test for the diagnosis of an acute thoracic spinal fractures. J Korean Soc Emerg Med. 2005. 16:1–5.2. Kaye M, Silverton S, Rosenthall L. Technetium-99m-pyrophosphate: studies in vivo and in vitro. J Nucl Med. 1975. 16:40–45.3. Kim BH, Im JI, Kim DJ, Park JY. Diganostic values of bone scan followed by CT scan in undetected pelvic bone fracture. J Korean Orthop Assoc. 1997. 32:523–529.
Article4. Kim HR, Thrall JH, Keyes JW Jr. Skeletal scintigraphy following incidental trauma. Radiology. 1979. 130:447–451.
Article5. Lee E, Worsley DF. Role of radionuclide imaging in the orthopedic patient. Orthop Clin North Am. 2006. 37:485–501.
Article6. Matheson GO, Clement DB, McKenzie DC, Taunton JE, Lloyd-Smith DR, MacIntyre JG. Stress fractures in athletes. A study of 320 cases. Am J Sports Med. 1987. 15:46–58.7. Matin P. The appearance of bone scans following fractures, including immediate and long-term studies. J Nucl Med. 1979. 20:1227–1231.8. Milgrom C, Chisin R, Giladi M, et al. Negative bone scans in impending tibial stress fractures. A report of three cases. Am J Sports Med. 1984. 12:488–491.
Article9. Scott S, Alazraki N, Manaster B. Failure of bone scanning to detect fractures in a woman on chronic steroid therapy. Skeletal Radiol. 1984. 12:204–207.
Article10. Sterling JC, Webb RF Jr, Meyers MC, Calvo RD. False negative bone scan in a female runner. Med Sci Sports Exerc. 1993. 25:179–185.
Article11. Subramanian G, McAfee JG. A new complex of 99mTc for skeletal imaging. Radiology. 1971. 99:192–196.12. Wen DY, Propeck T, Singh A. Femoral neck stress injury with negative bone scan. J Am Board Fam Pract. 2003. 16:170–174.
Article13. Yao L, Lee JK. Occult intraosseous fracture: detection with MR imaging. Radiology. 1988. 167:749–751.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- False negative bone scan finding of vertebral metastatic compression fracture: A case report
- The Significance of Bone Scan in Trauma in Orthopaedic Field
- Availability of Bone Scan in Chest Trauma Patients
- The Clinical Signifiance of Bone Scan in Fracture Diagnosis
- Acute New Compression Fractures of Consecutive Vertebral Bodies Adjacent to the Previously Augmented Level with Kyphoplasty
