A Case of Intestinal Duplication Cyst Identified as Pathological Lead Point in a Child with Recurrent Intussusception
- Affiliations
-
- 1Department of Pediatrics, College of Medicine, Dankook University, Cheonan, Korea. pdlks@hanmail.net
- 2Department of Pathology, College of Medicine, Dankook University, Cheonan, Korea.
- 3Department of Radiology, College of Medicine, Dankook University, Cheonan, Korea.
- KMID: 1459448
- DOI: http://doi.org/10.5223/kjpgn.2010.13.1.75
Abstract
- Intestinal duplication cysts are characterized by the attachment to some part of the gastrointestinal tract with which a blood supply is shared, and have an epithelial lining resembling some part of the alimentary tract. A 15-month-old female was admitted to our hospital with cyclic irritability, vomiting, and blood-tinged stool. The results of an ultrasound showed an ileocolic intussusception and a 1.3 cm cystic mass had double-wall sign and a Y-configuration with an adjacent ileal loop. She had a past history of two ileocolic intussusceptions. The cystic mass was considered to be a pathologic lead point, so resection and end-to-end anastomosis was performed. The gross and histologic evaluation of the specimen demonstrated a 2.4x2.4 cm cystic mass containing yellow mucoid fluid and the cyst wall was lined with intestinal and gastric mucosa and enclosed by a layer of muscle, which was shared with the adjacent ileum.
Keyword
MeSH Terms
Figure
-
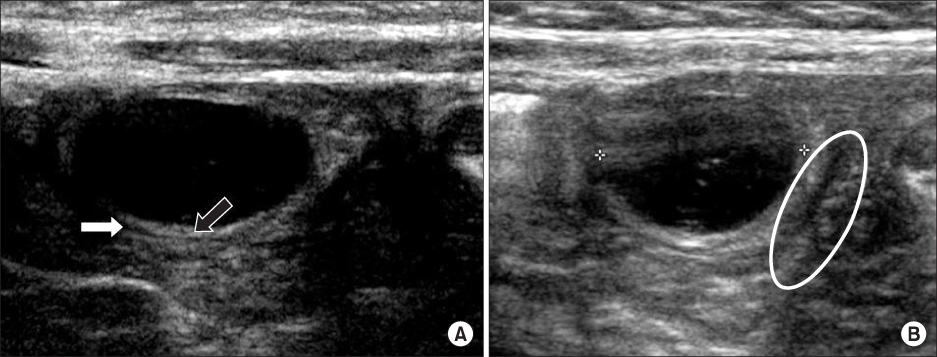
Fig. 1 (A) Ultrasound shows a cystic mass with a double-layered wall consisting of an echogenic inner layer (black arrow) and a hypoechoic outer layer (white arrow). (B) A Y-configuration is shown at the junction of the cyst and adjacent small bowel (oval line).

Fig. 2 On a contrast-enhanced CT scan, a 2.4 cm cystic-like mass with an enhancing wall (arrow) is demonstrated in the left lower peritoneal cavity adjacent to an ileal loop.

Fig. 3 The gross specimen demonstrates a 2.4×2.4 cm cystic mass adjacent to an ileal loop.

Fig. 4 (A) Low-power histologic photomicrograph demonstrates the cyst with a layer of muscle (arrowhead) is shared with adjacent ileum, and the white box represents a low magnification lesion of (B) (H&E, ×12.5). (B) The cystic outer wall is lined with shared normal intestinal mucosa (yellow arrow) and the inner wall is lined with ectopic gastric mucosa (black arrow; H&E, ×40).

Fig. 5 The cystic wall consists of inner hyperechoic and outer hypoechoic layers, known as the double-wall sign, and two Y-configurations (white line) are visible at the junctions of the cyst and adjacent small bowel loop (ref. 14).
Reference
-
1. Lee SH, Kim KH, Jung SE, Lee SC, Park KW, Kim WK. Clinical Characteristics and Management of Congenital Intestinal Duplication. J Korean Surg Soc. 2001. 61:530–536.2. Park SY, Park JY. Intestinal Duplication in Childhood. J Korean Surg Soc. 2008. 75:262–267.3. Kim HK, Woo ZH, Sohn JH. A report of 2 cases of duplication of the alimentary tract. J Korean Surg Soc. 1971. 13:456–459.4. Choi GW, Kang GS, Park BU, Lee WM, Jeen YS, Lee TW. A case ileal duplication with intussusception. J Korean Pediatr Soc. 1992. 35:563–568.5. Cheng G, Soboleski D, Daneman A, Poenaru D, Hurlbut D. Sonographic pitfalls in the diagnosis of enteric duplication cysts. AJR Am J Roentgenol. 2005. 184:521–525.
Article6. Milbrandt K, Sigalet D. Intussusception associated with a Meckel's diverticulum and a duplication cyst. J Pediatr Surg. 2008. 43:e21–e23.
Article7. Srivastava P, Gangopadhyay AN, Kumar V, Upadhyaya VD, Sharma SP, Jaiman R, et al. Noncommunicating isolated enteric duplication cyst in childhood. J Pediatr Surg. 2009. 44:e9–e10.
Article8. Chung JY, Park DC. A Case of Intra-Abdominal Esophageal Duplication Cyst. Korean J Pediatr Gastroenterol Nutr. 2001. 4:224–227.
Article9. Navarro O, Daneman A. Intussusception. Part 3: Diagnosis and management of those with an identifiable or predisposing cause and those that reduce spontaneously. Pediatr Radiol. 2004. 34:305–312.10. Lee KS, Park YJ. Clinical analysis of recurrent intussusception and the pathologic lead point in a single center. Korean J Pediatr Gastroenterol Nutr. 2009. 12:163–170.
Article11. De Roeck A, Vervloessem D, Mattelaer C, Schwagten K. Isolated enteric duplication cyst with respiratory epithelium: case report and review of the literature. Eur J Pediatr Surg. 2008. 18:337–339.
Article12. Kim YJ, Kim YK, Jeong YJ, Moon WS, Gwak HJ. Ileal duplication cyst: Y-configuration on in vivo sonography. J Pediatr Surg. 2009. 44:1462–1464.
Article13. Dias AR, Lopes RI, do Couto RC, Bonafe WW, D'Angelo L, Salvestro ML. Ileal duplication causing recurrent intussusception. J Surg Educ. 2007. 64:51–53.
Article14. Kim TW, Jung PM. A clinical study of intestinal duplication. J Korean Assoc Pediatr Surg. 2004. 10:9–16.
Article15. Schalamon J, Schleef J, Hollwarth ME. Experience with gastro-intestinal duplications in childhood. Langenbecks Arch Surg. 2000. 385:402–405.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Duodenal Duplication Cyst that Manifested as Duodeno-jejunal Intussusception in an Adult: A Case Report
- Clinical Analysis of Recurrent Intussusception and the Pathologic Lead Point in a Single Center
- Coincident Occurrence of Intestinal Duplication Cyst and Type I and Type II Intestinal Atresias
- Giant Duplication Cyst Presenting as a Discharging Umbilicus
- A Case of Intussusception Caused by Meckel's Diverticulum with Heterotopic Pancreatic and Gastric Tissues
