A Case of Obstructive Jaundice Secondary to Traumatic Pancreatitis Treated with Percutaneous Transhepatic Biliary Drainage
- Affiliations
-
- 1Department of Pediatrics, Gyeongsang National University School of Medicine, Gyeongsang Institute of Health Science, Jinju, Korea. hsyoun@gnu.ac.kr
- 2Department of Radiology, Gyeongsang National University School of Medicine, Gyeongsang Institute of Health Science, Jinju, Korea.
- KMID: 1459437
- DOI: http://doi.org/10.5223/kjpgn.2010.13.2.204
Abstract
- Isolated pancreatic trauma and secondary obstructive jaundice in the pediatric population is unusual. Biliary tract obstruction can be a major cause of acute pancreatitis. We report a case of obstructive jaundice secondary to isolated traumatic acute pancreatitis in a previously healthy 32-month-old girl. In our case, secondary obstructive jaundice aggravated the pancreatic inflammation and was successfully treated with percutaneous transhepatic biliary drainage (PTBD).
Keyword
Figure
-

Fig. 1 Whole abdominal computed tomography was performed on admission (A, B) showing diffuse pancreatic swelling and peripancreatic fluid collection (arrows), a relatively intact common bile duct (solid arrow), and a part of the gallbladder (dotted arrow), and 10 days after admission (C) showing intra- and extra-hepatic biliary duct dilatation (arrow) and milder pancreatic swelling and a decreased amount of peripancreatic fluid collection than before.
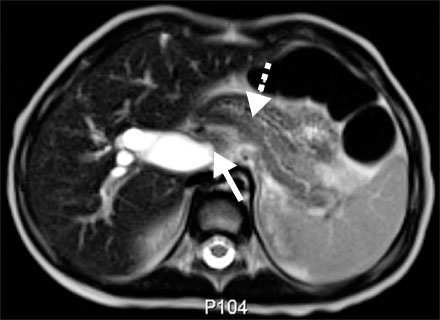
Fig. 2 Magnetic resonance cholangiopancreaticography was performed 28 days after admission showing a distended gallbladder, dilated biliary trees, and pancreatic duct (dotted arrow) and low signal lesion suggestive of a biliary stone in the distal common bile duct (solid arrow) and biliary sludge in the gallbladder.
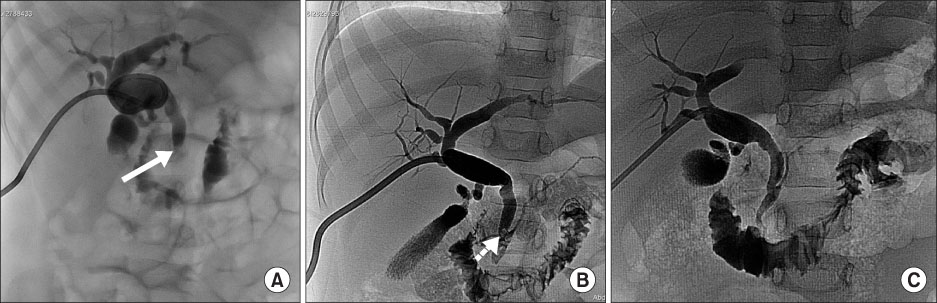
Fig. 3 Cholangiograms through the percutaneous transhepatic biliary drainage catheter were performed 33 days after admission (A) showing marked dilated intra- and extra-hepatic bile ducts, and a smooth, tapering biliary stricture in the distal common bile duct (solid arrow), and 35 days after admission (B) showing a mild dilated pancreatic duct and a filling defect (dotted arrow) in the distal common bile duct suggestive of a biliary stone which was removed by a skilled interventional radiologist via a stone basket and shown to be a small amount of biliary sludge, and 66 days after admission (C) showing no biliary dilatation or stricture of the common bile duct with free flow of contrast media from the common bile duct to the second portion of the duodenum.
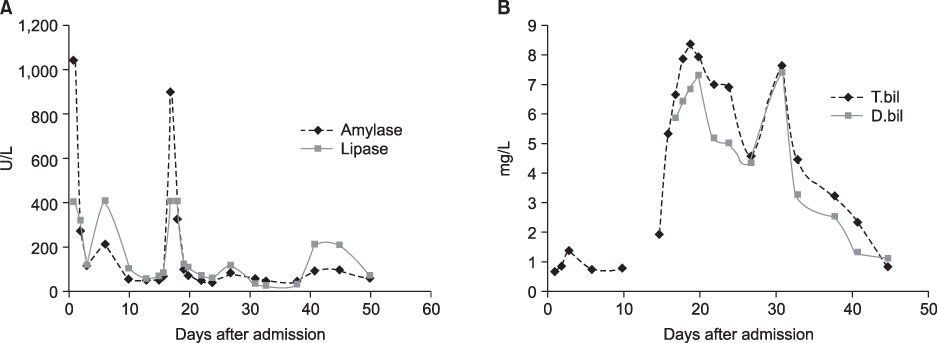
Fig. 4 Serial changes of laboratory findings, (A) serum amylase and lipase, (B) serum total bilirubin and direct bilirubin according to days after admission show temporal relationsship with (A) and (B).
Cited by 1 articles
-
Percutaneous Transhepatic Biliary Drainage in a Two-Month-Old Infant with Inspissated Bile Syndrome
Sung Hui Chang, Seung-Moon Joo, Choon-Sik Yoon, Kwang-Hun Lee, Soon Min Lee
Yonsei Med J. 2018;59(7):904-907. doi: 10.3349/ymj.2018.59.7.904.
Reference
-
1. Lopez MJ. The changing incidence of acute pancreatitis in children: a single-institution perspective. J Pediatr. 2002. 140:622–624.
Article2. Werlin SL, Kugathasan S, Frautschy BC. Pancreatitis in children. J Pediatr Gastroenterol Nutr. 2003. 37:591–595.
Article3. Moore EE, Cogbill TH, Malangoni MA, Jurkovich GJ, Shackford SR, Champion HR, et al. Organ injury scaling. Surg Clin North Am. 1995. 75:293–303.
Article4. Stringer MD. Pancreatitis and pancreatic trauma. Semin Pediatr Surg. 2005. 14:239–246.
Article5. Mattix KD, Tataria M, Holmes J, Kristoffersen K, Brown R, Groner J, et al. Pediatric pancreatic trauma: predictors of nonoperative management failure and associated outcomes. J Pediatr Surg. 2007. 42:340–344.
Article6. Benifla M, Weizman Z. Acute pancreatitis in childhood analysis of literature data. J Clin Gastroenterol. 2003. 37:169–172.7. Wood JH, Partrick DA, Bruny JL, Sauaia A, Moulton SL. Operative vs nonoperative management of blunt pancreatic trauma in children. J Pediatr Surg. 2010. 45:401–406.
Article8. Dryburgh PR, White JAM. Late obstruction of the intrahepatic common bile duct after seat-belt injury. S Afr Med J. 1980. 58:534–535.9. Choi BH, Lim YJ, Yoon CH, Kim EA, Park YS, Kim KM. Acute pancreatitis associated with biliary disease in children. J Gastroenterol Hepatol. 2003. 18:915–921.
Article10. Ko JS. Fibrosing pancreatitis causing obstructive jaundice. Korean J Gastroenterol. 2008. 52:271–272.11. Yachha SK, Chetri K, Saraswat VA, Baijal SS, Sikora SS, Lal R, et al. Management of childhood pancreatic disorders: a multidisciplinary approach. J Pediatr Gastroenterol Nutr. 2003. 36:206–212.
Article12. Sylvester FA, Shucktt B, Cutz E, Durie PR, Marcon MA. Management of fibrosing pancreatitis in children presenting with obstructive jaundice. Gut. 1998. 43:715–720.
Article13. Wales PW, Shuckett B, Kim PCW. Long-term outcome after nonoperative management of complete traumatic pancreatic transection in children. J Pediatr Surg. 2001. 36:823–827.
Article14. Delcenserie R, Joly JP, Lenne C, Kannoun MM, Sevestre H, Capron JP, et al. Fibrotic stricture of the extrapancreatic biliary tract: a new complication of acute pancreatitis. Two cases. Pancreas. 1995. 10:100–103.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Percutaneous transhepatic biliary drainage
- Percutaneous Transhepatic Transtumoral Biliary Drainage in a Patient with Obstructive Jaundice Due to Klatskin Tumor
- A clinical analysis of percutaneous transhepatic biliary drainage in the patients with obstructive jaundice
- Ultrasonography in obstructive jaundice : a comparison with percutaneous transhepatic cholangiography
- Significance of preoperative percutaneous transhepatic biliary drainage(PTBD) in obstructive jaundice
