Sclerotherapy of benign oral vascular lesion with sodium tetradecyl sulfate: cases report
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, College of Dentistry, Dankook University, Choenan, Korea. kkwoms@dku.edu
- KMID: 1457780
- DOI: http://doi.org/10.5125/jkaoms.2010.36.4.280
Abstract
- Hemangioma and vascular malformation is a common vascular benign lesion in the head and neck region. The lesion is a congenital malformation observed in neonates. The treatment this lesion includes surgical excision, cryotherapy, selective embolization and treatment with sclerotic agents. We present three cases of benign oral vascular lesions treated with an intralesional injection of sodium tetradecyl sulfate. The lesions virtually disappeared after three sessions of sclerotherapy, leaving an inconspicuous scar. No side effects were observed. Sclerotherapy with sodium tetradecyl sulfate is effective in treating benign oral vascular lesions, and the use of the sodium tetradecyl sulfate provides alternative or support for surgical methods.
Keyword
MeSH Terms
Figure
-

Fig. 1. Bluish lesion on the labial mucosa of 1-year-old male before sclerotherapy.
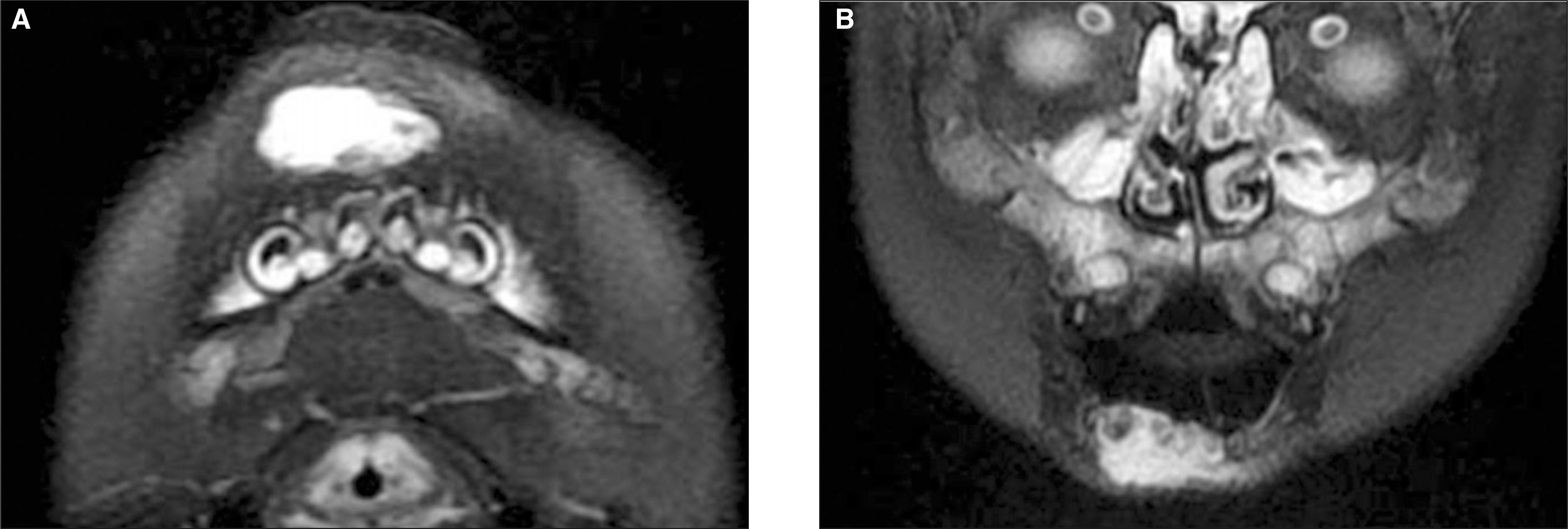
Fig. 2. Increased signal intensity is shown on the lesion area. A. Preoperative MRI T2W1 axial view, B. Preoperative MRI T2W1 coronal view.(MRI: magnetic resonance imaging)

Fig. 3. Three weeks after the injection of sodium tetradecyl sulfate. The lesion regressed almost completely.

Fig. 4. Bluish macular lesion on the right buccal mucosa of 9-year-old male before injection.
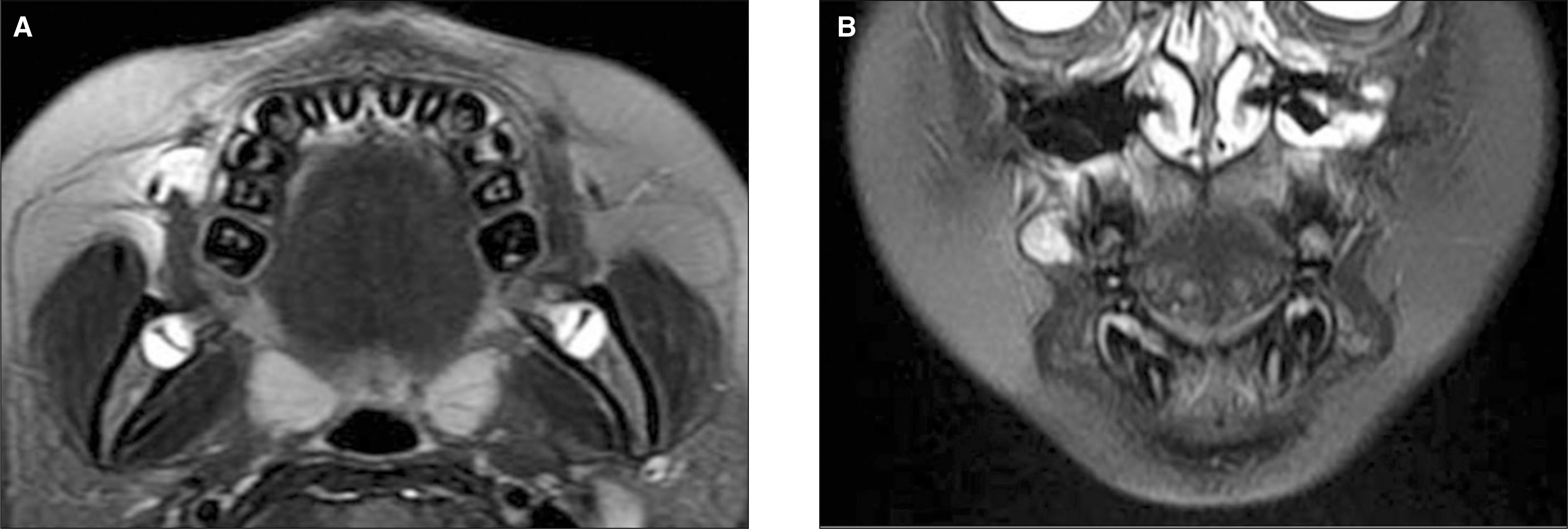
Fig. 5. High signal is seen on the right buccal mucosa. A. Preoperative MRI T2W1 axial view, B. Preoperative MRI T2W1 coronal view.
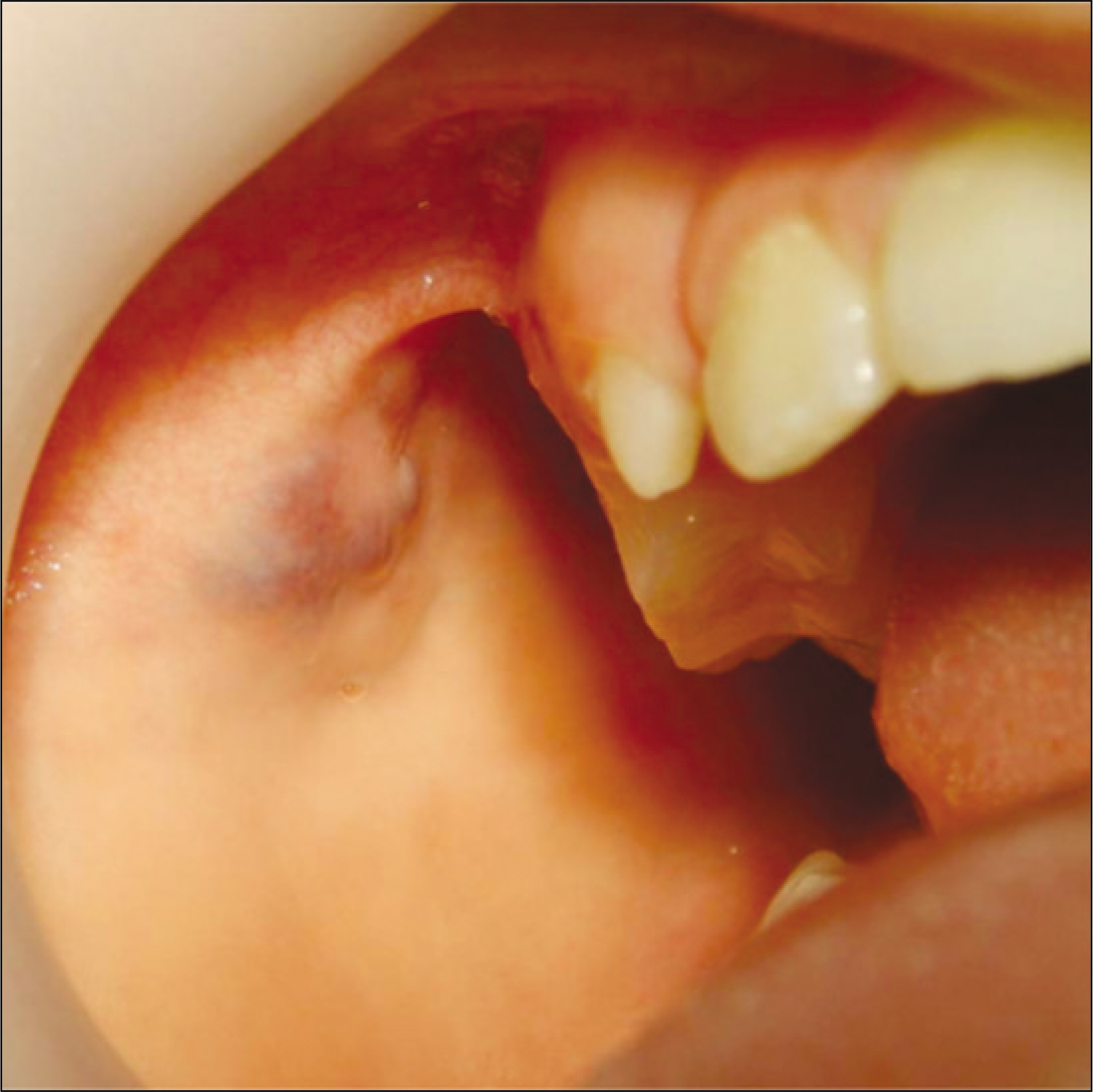
Fig. 6. Four weeks after initial sclerotherapy.

Fig. 7. Two weeks after the second injection of sclerosant. The lesion regressed, leaving an inconspicuous scar.
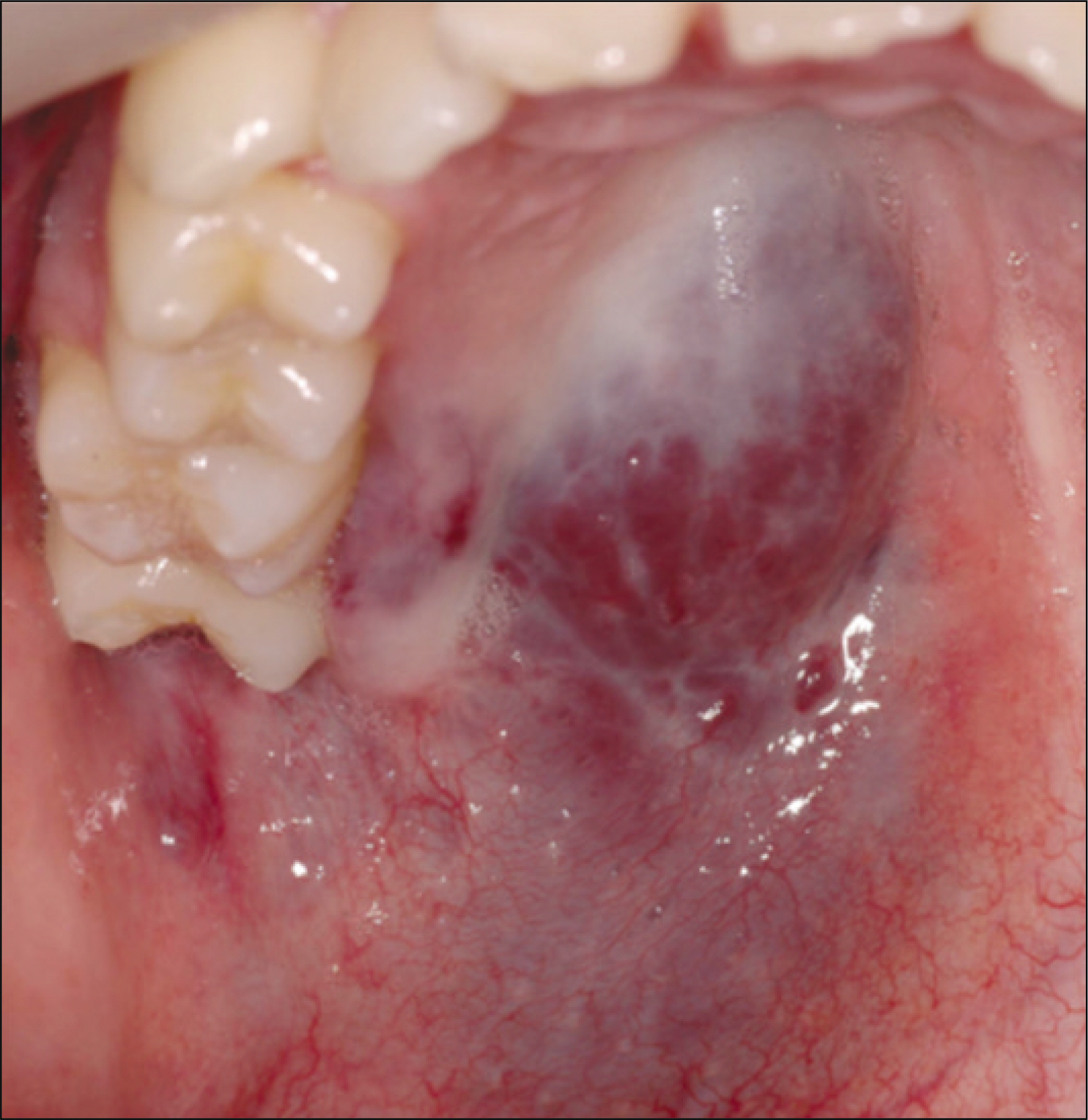
Fig. 8. Large vascular lesion on the palate of 22-year-old male before sclerotherapy.
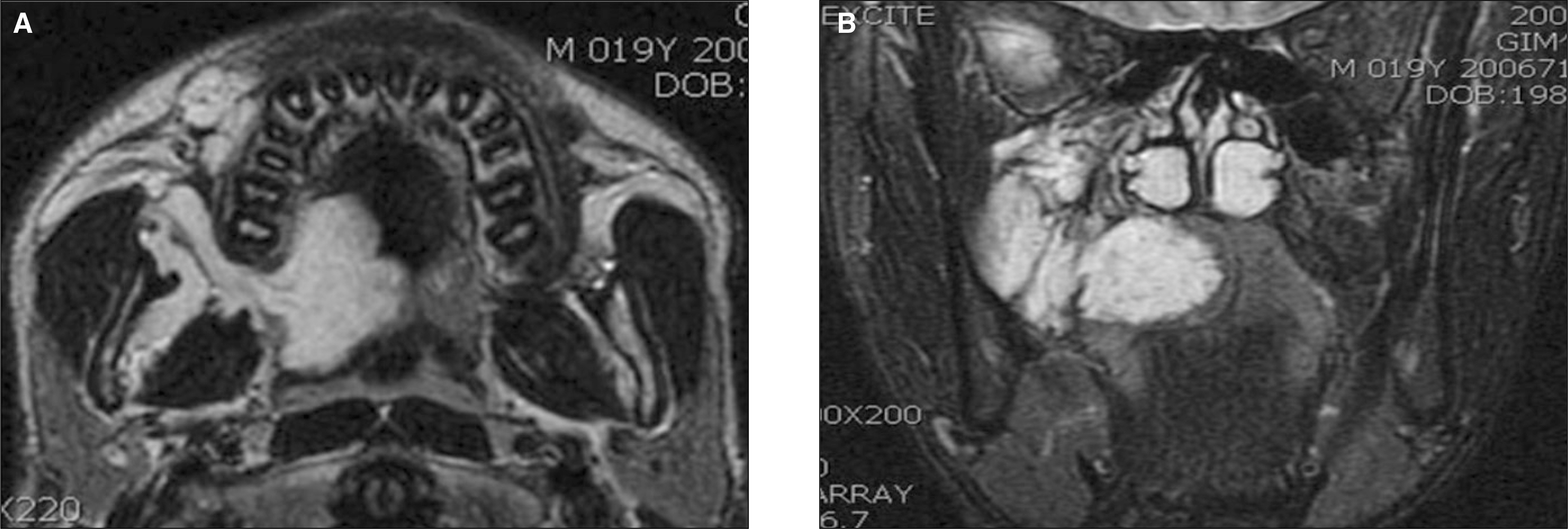
Fig. 9. High intensity is seen on the lesion area. The lesion involved hard and soft palate and buccal mucosa. A. Preoperative MRI T2W1 axial view, B. Preoperative MRI T2W1 coronal view.

Fig. 10. Three weeks after initial sclerotherapy.

Fig. 11. Four weeks after second sclerotherapy. Recovery of normal color and surface texture is seen.

Fig. 12. The lesion regressed considerably, but small signal void is observed in central area of the lesion. A. Postoperative MRI T2W1 axial view, B. Postoperative MRI T2W1 coronal view.
Cited by 1 articles
-
Intramuscular hemangioma formation in the masseter muscle: a case report
Hyun-Woo Kim, Tae-Jun Kil, Jong-Myung Choi, Woong Nam, In-Ho Cha, Hyung-Jun Kim
J Korean Assoc Oral Maxillofac Surg. 2010;36(5):423-426. doi: 10.5125/jkaoms.2010.36.5.423.
Reference
-
References
1. Finn MC, Glowack J, Mulliken JB. Congenital vascular lesions: clinical application of a new classification. J Pediatr Surg. 1983; 18:894–900.2. Mulliken JB, Glowacki J. Hemangiomas and vascular malformations in infants and children: a classification based on endothelial characteristics. Plastic Reconstr Surg. 1982; 69:412–22.3. Johann AC, Aguiar MC, do Carmo MA, Gomez RS, Castro WH, Mesquita RA. Sclerotherapy of benign oral vascular lesion with ethanolamine oleate: an open clinical trial with 30 lesions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005; 100:579–84.4. Tyagi I, Syal R, Goyal A. Management of low-flow vascular malformations of upper aero digestive system-role of N-butyl cyanoacrylate in peroperative devascularization. Br J Oral Maxillofac Surg. 2006; 44:152–6.
Article5. Baurmash H, de Chiara S. A conservative approach to the management of orofacial vascular lesions in infants and children: report of cases. J Oral Maxillofac Surg. 1991; 49:1222–5.
Article6. Ethunandan M, Mellor TK. Haemangiomas and vascular malformations of the maxillofacial region-a review. Br J Oral Maxillofac Surg. 2006; 44:263–72.
Article7. de Lorimier AA. Sclerotherapy for venous malformations. J Pediatr Surg. 1995; 30:188–93.
Article8. Calonje E, Fletcher CDM. Tumors of blood vessels and lymphatics. Fletcher CDM, editor. Diagnostic histopathology of tumors. New York: Churchill Livingstone;1995. p. 43–78.9. Jayakumar PN, Desai SV, Kovoor JM, Vasudev MK. Percutaneous embolization of mandibular hemangioma: a case report. J Oral Maxillofac Surg. 2002; 60:945–8.
Article10. Muto T, Kinehara M, Takahara M, Sato K. Therapeutic embolization of oral hemangiomas with absolute ethanol. J Oral Maxillofac Surg. 1990; 48:85–8.
Article11. Tanaka T, Morimoto Y, Takano H, Tominaga K, Kito S, Okabe S, et al. Three-dimensional identification of hemangiomas and feeding arteries in the head and neck region using combined phase-contrast MR angiography and fast asymmetric spin-echo sequences. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005; 100:609–13.
Article12. Baurmash H, Mandel L. The nonsurgical treatment of hemangioma with Sotradecol. Oral Surg Oral Med Oral Pathol. 1963; 16:777–82.
Article13. Sadeghi E, Gingrass D. Oral hemangioma treated with a sclerosing agent. Report of a case. Int J Oral Maxillofac Surg. 1989; 18:262–3.14. Minkow B, Laufer D, Gutman D. Treatment of oral hemangiomas with local sclerosing agents. Int J Oral Surg. 1979; 8:18–21.
Article15. Sadeghi E, Gingrass D. Histophatologic appraisal of an oral hemangioma treated with a sclerosing agent. Compendium. 1991; 12:288–90.16. Matsumoto K, Nakanishi H, Koizumi Y, Seike T, Kanda I, Kubo Y. Sclerotherapy of hemangioma with late involution. Dermatol Surg. 2003; 29:668–71.
Article17. Christensen RW. The treatment of oral hemangiomas: report of four cases. Oral Surg Oral Med Oral Pathol. 1959; 12:912–21.18. Choi YH, Han MH, O-Ki K, Cha SH, Chang KH. Craniofacial cavernous venous malformations: percutaneous sclerotherapy with use of ethanolamine oleate. J Vasc Interv Radiol. 2002; 13:475–82.19. Kuo HW, Yang CH. Venous lake of the lip treated with a sclerosing agent: report of two cases. Dermatol Surg. 2003; 29:425–8.
Article20. Salins PC, Kumar S, Rao CB. Management of large vascular lesions of the lip: case reports. Int J Oral Maxillofac Surg. 1997; 26:45–8.
Article21. van Doorne L, Maeseneer M, Stricker C, Vanrensbergen R, Stricker M. Diagnosis and treatment of vascular lesions of the lip. Br J Oral Maxillofac Surg. 2002; 40:497–503.
Article22. Fishman SJ, Mulliken JB. Hemangiomas and vascular malformations of infancy and childhood. Pediatr Clin North Am. 1993; 40:1177–200.
Article23. Chin DC. Treatment of maxillary hemangioma with a sclerosing agent. Oral Surg Oral Med Oral Pathol. 1983; 55:247–9.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Sclerotherapy using 1% sodium tetradecyl sulfate to treat a vascular malformation: a report of two cases
- Utility of sodium tetradecyl sulfate sclerotherapy from benign oral vascular lesion
- A Case of Glomangioma Treated with Sclerotherapy
- Three Cases of Digital Mucous Cyst Treated with Sodium Tetradecyl Sulfate Sclerotherapy
- A Case of Linear Digital Mucous Cyst Successfully Treated with 1% Sodium Tetradecyl Sulfate Intralesional Proximal End Injection
