Lower Cervical Spine Injury
- KMID: 1449426
- DOI: http://doi.org/10.12671/jkfs.2011.24.1.100
Abstract
- No abstract available.
MeSH Terms
Figure
-
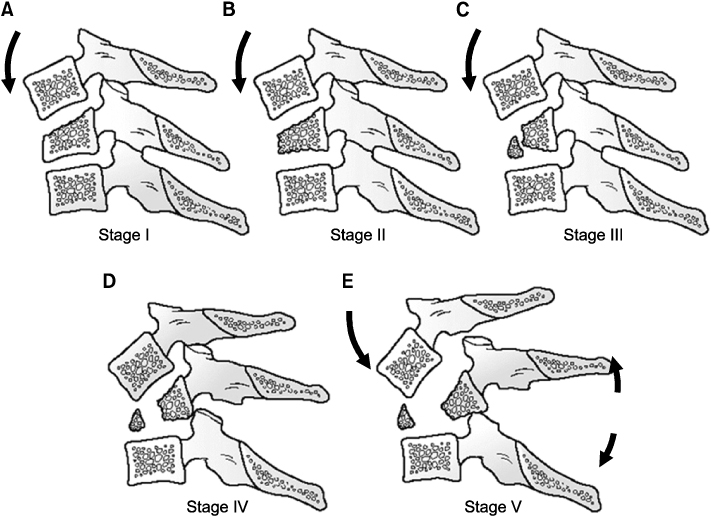
Fig. 1 Compressive flexion (CF) injuries are divided into five stages. The injury is speculated to occur first by flexion of the spine through the facet joints. The anterior column (vertebral body) becomes increasingly compressed and shortened. Eventually, the PLC fails, noted by interspinous gapping and local kyphosis. With further energy, the facet joints will fail, leading to translational deformity. (A) CF Stage I: Blunting of the anterosuperior vertebral body margin. (B) CF Stage II: Beak-appearance of the anterosuperior vertebral body margin, a sagittal vertebral body split may also be present. (C) CF Stage III: Oblique primary fracture line that extends from the anterior vertebral body to the inferior endplate (This has been subsequently described by other authors as a so-called tear-drop fracture.). (D) CF Stage IV: In addition to stage 3 features, posterior translation of the upper vertebra measuring less than 3 mm. (E) CF Stage V: Posterior translation of the upper vertebral measuring 3 mm or greater, facet gapping, indicating anterior and posterior ligamentous injury.
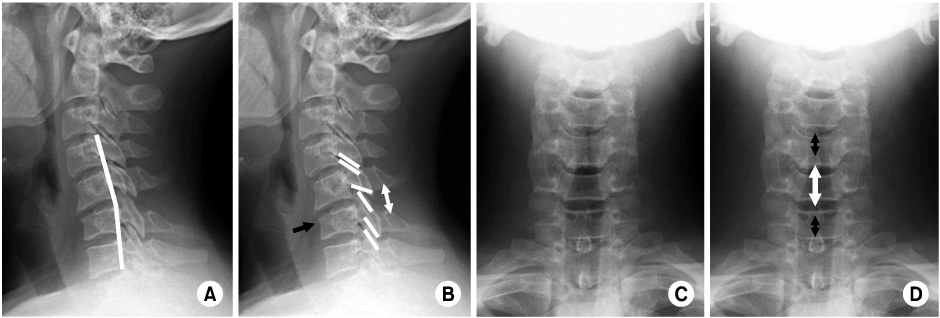
Fig. 2 Anterior subluxation of C5 with wedge compression fracture of C6. (A, B) Lateral radiographs of the cervical spine show incongruity and lack of parallelism of the C5-6 facets (white lines in B), exposure of the superior facet joint surface of C6, and widening of the interspinous distance at C5-6 ("fanning") (white arrow in B) relative to adjacent levels. Note the subtle localized hyperkyphotic angulation at C5-6 (white lines in A). There is loss of anterior stature of the body of C6 secondary to the compression fracture involving its superior end plate (black line in B). (C, D) AP radiographs of the cervical spine. On the frontal projection the C5-6 interspinous space is abnormally wide (white arrow in D). This represents the "fanning" seen on the lateral radiograph.
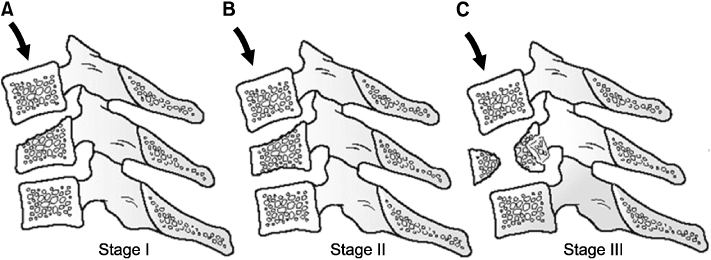
Fig. 3 Vertical compressive (VC) lesions are thought to arise from primarily axial loads to the cervical spine. The final stage of the injury may result from flexion or extension vectors, which ultimately produce posterior or anterior ligamentous injury, respectively. (A) VC Stage I: Central superior or inferior endplate fracture. (B) VC Stage II: Superior and inferior endplate fractures, sometimes with vertebral body fracture lines that give the appearance of a quadrangular fracture fragment. (C) VC Stage III: Vertebral body comminution, with or without retropulsion of fragments (This has been by others as a burst-type cervical fracture), with or without kyphotic (late flexion type) or translational (late extension type) deformity.

Fig. 4 Burst (dispersion, axial loading) fracture of C5. Lateral radiograph (A) and sagittal multiplanar reformation (B) demonstrate fractures of each end plate (white arrows) with both anterior and posterior displacement of fracture fragments (black arrows), the latter into the central spinal canal. Note the typical straight alignment of the cervical spine in patients with burst fractures. (C) Coronal multiplanar CT reformation shows vertical fracture lines extending through the midportion of the vertebral bodies of C5 and C6 with widening of suprajacent (white line) and narrowing of subjacent uncovertebral joints (black line) secondary to lateral displacement of hemivertebral fracture fragments (white double-headed arrow). (D, E) Axial CT images demonstrate a comminuted fracture of the vertebral body with fragment dispersion; there is a vertical body fracture (white arrows), fragment retropulsion into the spinal canal, and bilateral fractures at the junctions of the laminae and articular masses (black arrows).

Fig. 5 Distractive flexion (DF) injuries are thought to occur from primarily flexion injury vectors that rotate about an axis anterior to the vertebral body. Thus, distraction and failure of the posterior ligaments can occur without significant vertebral body fracture. In this injury group, increasingly higher stages does not always correspond to increasing amount of instability. (A) DF Stage I: Facet subluxation, gapping of the spinous process ligaments, indicating failure of the PLC, with or without some blunting of anterosuperior vertebral body (like CF stage I). (B) DF Stage II: Unilateral facet dislocation, usually PLC is intact, rotational deformity. (C) DF Stage III: Bilateral facet dislocations, 50% translation of upper vertebral body on lower one. (D) DF Stage IV: Close to 100% translation of upper vertebral body on lower one, apperance of a so-called floating vertebra.
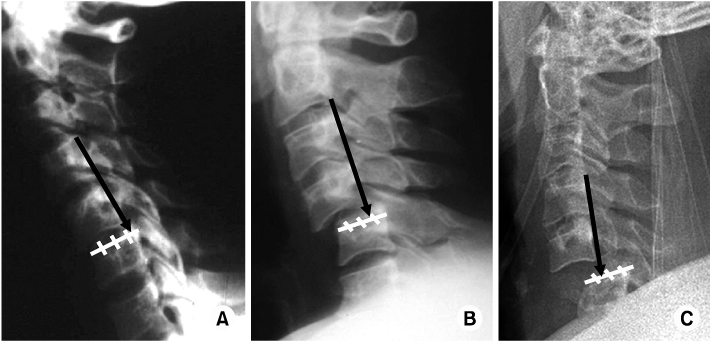
Fig. 6 Anterior vertebral translation in different flexion injuries. The amount of anterior translation with unilateral dislocation (B) is less than occurs with bilateral facet dislocation (C) but greater than that of anterior subluxation (A). (A) In anterior subluxation the involved vertebra may be displaced slightly anteriorly (1 to 3 mm), <25% of the AP diameter of the subjacent vertebral body. (B) Unilateral facet dislocation demonstrating anterior translation of the dislocated vertebra 25% to 50% of the AP diameter of the subjacent vertebral body. (C) Bilateral facet dislocation with anterior displacement of the involved vertebra >50% of the anteroposterior diameter of the subjacent vertebral body.
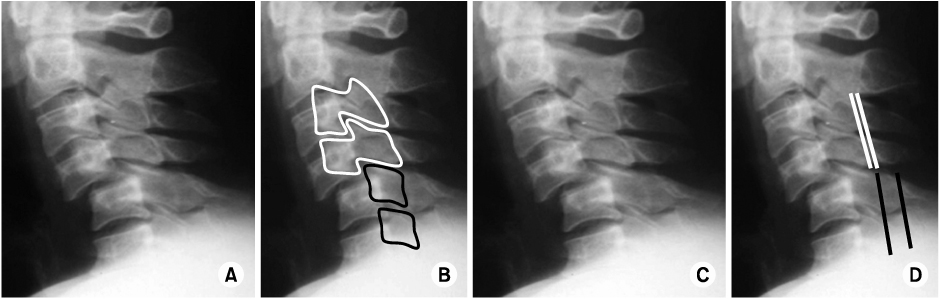
Fig. 7 "Bowtie" and "laminar space" (114) signs in unilateral facet dislocation of C4-5. (A, B) Lateral cervical spine radiographs show anterolisthesis of C4-5 with about 25% displacement. The articular pillars are offset from C4 above (white lines in B) and are seen in oblique profile giving the "bowtie" appearance; the "bowtie" sign indicates rotation. The articular pillars are superimposed at C5 and below and are seen in lateral profile (black lines in B). (C, D) Lateral cervical spine radiographs. The laminar space is the distance between the spinolaminar line and the posterior surface of the articular pillars. The laminar space changes abruptly between C4 and C5, with the laminar space reduced above the C5 level (compare the black lines and white lines in D indicating sudden rotation).
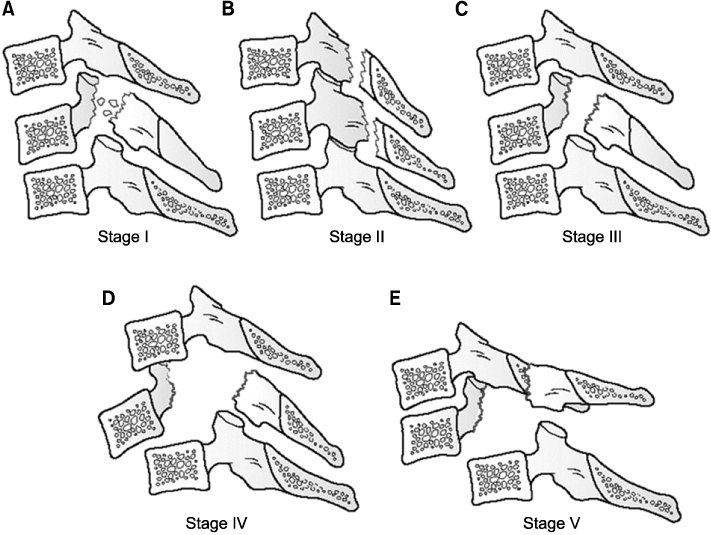
Fig. 8 Compressive extension (CE) injuries are divided into five stages. They are postulated to start with compression of the posterior elements without failure of the anterior ligaments. Further injury leads to failure of the anterior/posterior ligaments. (A) CE Stage I: Posterior arch fracture that may be facet, pedicle, or lamina fracture, with or without rotation that can result in mild anterior translation. (These are more commonly referred to as lateral mass fractures.) (B) CE Stage II: Bilateral lamina fractures, can be multiple levels. (C) CE Stage III: Bilateral lamina, facet, pedicle fractures without vertebral body displacement. Although admittedly "hypothetical… having not been encountered" in their review, the injury may be described as a floating lateral mass fracture. (D) CE Stage IV: As for CF stage III, with partial anterior vertebral body displacement. (E) CE Stage V: As for CF stage III, with 100% anterior vertebral body displacement.

Fig. 9 Hyperextension comminuted laminar and spinous processes fractures. Cervical spine injuries caused by hyperextension are characterized by distraction of the anterior and middle columns and compression of the posterior column (A). Lateral radiograph demonstrates posterior impaction with multiple comminuted laminar and spinous processes fractures from C2 to C6 (white arrows). The acute vacuum disc (black arrow) with abnormal widening of the anterior C6-7 disc space is a sign of anterior and middle column distraction. (B, C) Axial CT images demonstrate displacement of the spinous processes and bilateral comminuted laminar fractures (white arrows).
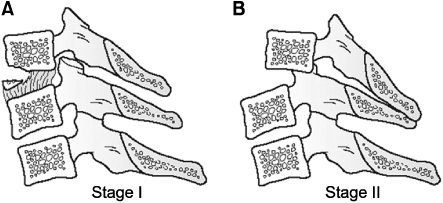
Fig. 10 Distractive extension (DE) injuries, like DF injuries, demonstrate substantial ligamentous injury in lower stages. Initial failure is through the anterior ligaments. (A) DE Stage I: Abnormal widening of the disc space, may or may not be avulsion fractures of the anterior vertebral body margin, no posterior translation. (B) DE Stage II: DF stage I plus posterior translation.
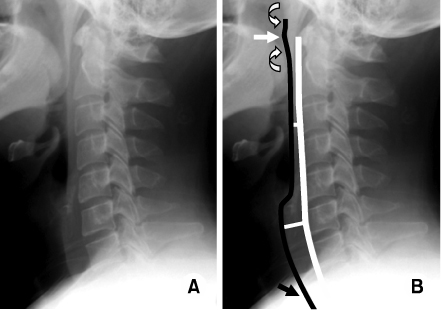
Fig. 11 Normal prevertebral soft tissues. Normal lateral radiographs (A, B). The prevertebral soft tissue is normal in thickness (white lines, C3 <5 mm and C6 <22 mm) and contour (black line). Note slight convex bulge anterior to C1 anterior tubercle (white arrow) and concavity caudal and rostral to the tubercle (curved arrows). At the cervicothoracic level the soft tissue shadow contour (black arrow) is normally near parallel to the arc formed by the anterior cortices of the lower cervical and upper thoracic vertebral bodies.
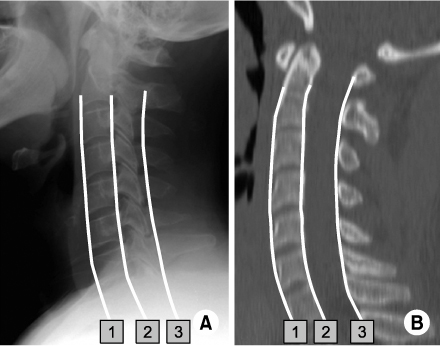
Fig. 12 Lateral radiograph (A) and sagittal CT multiplanar reformation (B) of a normal cervical spine. The vertebrae are aligned in a gentle lordotic configuration. The lines connecting the anterior margin of the vertebral bodies (1), the posterior cortical margins of the vertebral bodies (2), and the anterior margins of the junctions of the spinous processes and laminae (spinolaminar line) (3) should form three parallel gentle convex curves with no steps or discontinuities. The spacing between these lines is uniform.
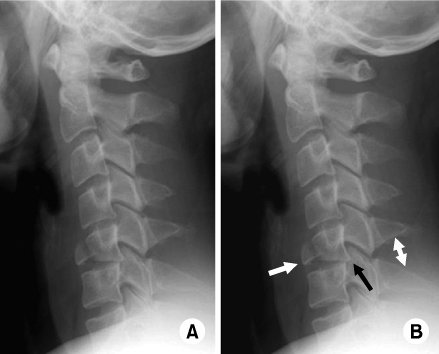
Fig. 13 Flexion teardrop fracture of C5. Lateral radiographs (A, B) of the cervical spine show typical flexion teardrop fracture with anteriorly displaced triangular fracture fragment ("teardrop") of the anterior-inferior aspect of vertebral body of C5 (white arrow in B) and retropulsion of its posterior vertebral body fragment into spinal canal (black arrow in B). Note a subtle localized kyphotic angulation at C5-6 and widening of the interspinous distance at C5-6 ("fanning") (white double arrow in B).

Fig. 14 C5-6 unilateral facet joint dislocation. Lateral radiographs (A) of the cervical spine show unilateral facet joint dislocation. Lateral radiographs (B) of the 2 years after operation (ACDF) show well reduction and fixation state.
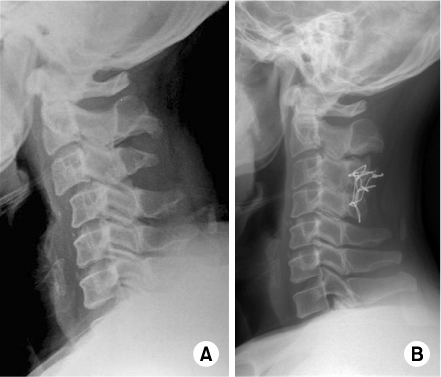
Fig. 15 C3-4 unilateral facet joint dislocation. Lateral radiographs (A) of the cervical spine show unilateral facet joint dislocation. Lateral radiographs (B) of the 3 years after operation (posterior wiring) show well reduction and fixation state.

Fig. 16 Bursting fracture of T1 and C7-T1 unilateral facet joint dislocation. Lateral radiographs (A) of the cervical spine show anterior wedging fracture of T1 and C7-T1 unilateral facet joint dislocation. Lateral radiographs (B) of the 6 months after operation (ACDF and posterior fusion with lateral mass screw) show well reduction and fixation state.
Reference
-
1. Aebi M, Zuber K, Marchesi D. Treatment of cervical spine injuries with anterior plating. Indications, techniques, and results. Spine (Phila Pa 1976). 1991. 16:3 Suppl. S38–S45.2. Ahn JS, Lee JK, Yang JY, Lee HH. Change of the lordosis on cervical spine after anterior interbody fusion with autogenous iliac strut bone graft. J Korean Soc Spine Surg. 2001. 8:468–474.
Article3. Allen BL Jr, Ferguson RL, Lehmann TR, O'Brien RP. A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine (Phila Pa 1976). 1982. 7:1–27.
Article4. Argenson C, Lovet J, Sanouiller JL, de Peretti F. Traumatic rotatory displacement of the lower cervical spine. Spine (Phila Pa 1976). 1988. 13:767–773.
Article5. Bohlman HH. Acute fractures and dislocations of the cervical spine. An analysis of three hundred hospitalized patients and review of the literature. J Bone Joint Surg Am. 1979. 61:1119–1142.
Article6. Born JD, Albert A, Hans P, Bonnal J. Relative prognostic value of best motor response and brain stem reflexes in patients with severe head injury. Neurosurgery. 1985. 16:595–601.
Article7. Braakman R, Vinken PJ. Unilateral facet interlocking in the lower cervical spine. J Bone Joint Surg Br. 1967. 49:249–257.
Article8. Calenoff L, Chessare JW, Rogers LF, Toerge J, Rosen JS. Multiple level spinal injuries: importance of early recognition. AJR Am J Roentgenol. 1978. 130:665–669.
Article9. Chung JY, Heo JP, Yi KT. Anterior plate fixation of the cervical spine fractures in ankylosing spondylitis. J Korean Soc Spine Surg. 1997. 4:106–113.10. Clark CR, Wessels WE. Unilateral cervical facet fracture-dislocation. Surg Rounds Orthop. 1987. 45:15–19.11. Cybulski GR, Douglas RA, Meyer PR Jr, Rovin RA. Complications in three-column cervical spine injuries requiring anterior-posterior stabilization. Spine (Phila Pa 1976). 1992. 17:253–256.
Article12. de Oliveira JC. Anterior reduction of interlocking facets in the lower cervical spine. Spine (Phila Pa 1976). 1979. 4:195–202.
Article13. Denis F. The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. Spine (Phila Pa 1976). 1983. 8:817–831.
Article14. Ducker TB, Bellegarrigue R, Salcman M, Walleck C. Timing of operative care in cervical spinal cord injury. Spine (Phila Pa 1976). 1984. 9:525–531.
Article15. Eismont FJ, Arena MJ, Green BA. Extrusion of an intervertebral disc associated with traumatic subluxation or dislocation of cervical facets. Case report. J Bone Joint Surg Am. 1991. 73:1555–1560.
Article16. Garfin SR, Botte MJ, Waters RL, Nickel VL. Complications in the use of the halo fixation device. J Bone Joint Surg Am. 1986. 68:320–325.
Article17. Harris WH, Hamblen DL, Ojemann RG. Traumatic disruption of cervical intervertebral disk from hyperextension injury. Clin Orthop Relat Res. 1968. 60:163–167.
Article18. Hwang BY, Song KJ, Ji JH. Disc extrusion on lower cervical facet joint fracture - dislocation. J Korean Orthop Assoc. 1997. 32:1078–1084.
Article19. Kornberg M. The computed tomographic appearance of a unilateral jumped cervical facet (the "false" facet joint sign). Spine (Phila Pa 1976). 1986. 11:1038–1040.
Article20. Kostuik JP. Indications for the use of the halo immobilization. Clin Orthop Relat Res. 1981. 154:46–50.
Article21. Maiman DJ, Barolat G, Larson SJ. Management of bilateral locked facets of the cervical spine. Neurosurgery. 1986. 18:542–547.
Article22. Marar BC. Hyperextension injuries of the cervical spine. The pathogenesis of damage to the spinal cord. J Bone Joint Surg Am. 1974. 56:1655–1662.23. Moon MS, Kim I, Kim OB. Anterior interbody fusion in unstable fracture and fracture-dislocation of the cervical spine. J Korean Orthop Assoc. 1981. 16:265–276.
Article24. Park HJ, Jeon JS, Lee PE. Range of motion of cervical spine in normal Korean people. J Korean Soc Spine Surg. 2004. 11:83–89.
Article25. Park HJ, Kim IG, Kim WK. Changes of adjacent segment in anterior cervical fusion. J Korean Soc Spine Surg. 2003. 10:269–276.
Article26. Plunkett PK, Redmond AD, Billsborough SH. Cervical subluxation: a deceptive soft tissue injury. J R Soc Med. 1987. 80:46–47.
Article27. Pratt ES, Green DA, Spengler DM. Herniated intervertebral discs associated with unstable spinal injuries. Spine (Phila Pa 1976). 1990. 15:662–666.
Article28. Richman JD, Daniel TE, Anderson DD, Miller PL, Douglas RA. Biomechanical evaluation of cervical spine stabilization methods using a porcine model. Spine (Phila Pa 1976). 1995. 20:2192–2197.
Article29. Rifkinson-Mann S, Mormino J, Sachdev VP. Subacute cervical spine instability. Surg Neurol. 1986. 26:413–416.
Article30. Rizzolo SJ, Piazza MR, Cotler JM, Balderston RA, Schaefer D, Flanders A. Intervertebral disc injury complicating cervical spine trauma. Spine (Phila Pa 1976). 1991. 16:6 Suppl. S187–S189.
Article31. Robertson PA, Ryan MD. Neurological deterioration after reduction of cervical subluxation. Mechanical compression by disc tissue. J Bone Joint Surg Br. 1992. 74:224–227.
Article32. Rorabeck CH, Rock MG, Hawkins RJ, Bourne RB. Unilateral facet dislocation of the cervical spine An analysis of the results of treatment in 26 patients. Spine (Phila Pa 1976). 1987. 12:23–27.33. Roy-Camille R, Saillant G, Mazel C. Internal fixation of the unstable cervical spine by a posterior osteosynthesis with plates and screws. The cervical spine. 1989. 2nd ed. Philadelphia: JB Lippincott;390–403.34. Song KJ, Lee KB. The prognosis of the acute cervical spinal cord injury. J Korean Orthop Assoc. 1998. 33:794–801.
Article35. Song KJ, Lee KR. The significance of space available for the spinal cord at the injured level in the lower cervical spine fractures and dislocations. J Korean Orthop Assoc. 1997. 32:1070–1077.
Article36. Song KJ, Shin PS. Surgical treatment of lower cervical spine injury. J Korean Orthop Assoc. 1999. 34:117–126.
Article37. Stauffer ES, Kelly EG. Fracture-dislocations of the cervical spine. Instability and recurrent deformity following treatment by anterior interbody fusion. J Bone Joint Surg Am. 1977. 59:45–48.
Article38. Vaccaro AR, Cook CM, McCullen G, Garfin SR. Cervical trauma: rationale for selecting the appropriate fusion technique. Orthop Clin North Am. 1998. 29:745–754.39. Webb JK, Broughton RB, McSweeney T, Park WM. Hidden flexion injury of the cervical spine. J Bone Joint Surg Br. 1976. 58:322–327.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pattern of Cervical Spine Injury in Patients with a Facial Fracture
- Missed Traumatic Cervical Spine Injury
- Posterior Cervical Plate Fixation in Cervical Injuries
- Clinical Analysis of Lower Cervical Spine-Injuried Patients
- Delayed or Missed Diagnosis of Cervical Instability after Traumatic Injury: Usefulness of Dynamic Flexion and Extension Radiographs
