Maxillary distraction osteogenesis in the management of cleft lip and palate: report of 2 cases
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, Ewha Womans University Mokdong Hospital, Ewha Womans University School of Medicine, Seoul, Korea. sjsj7777@ewha.ac.kr
- KMID: 1449065
- DOI: http://doi.org/10.5125/jkaoms.2011.37.4.321
Abstract
- This study is to evaluate the growth and development of the maxilla advanced by transoral distraction osteogenesis of cleft lip and palate children. Subjects are two patients diagnosed as maxillary hypoplasia with cleft lip and palate, and followed up over 5 years after distraction. At the age of 11.4 years (mean), the distraction had been rendered and periodically taken lateral cephalograms were analysed to trace the growth of the maxilla. This cephalometric study showed continuous growth and development of the distracted maxilla to be stable through long term follow-up.
MeSH Terms
Figure
-

Fig. 1. Clinical photographs at surgery.
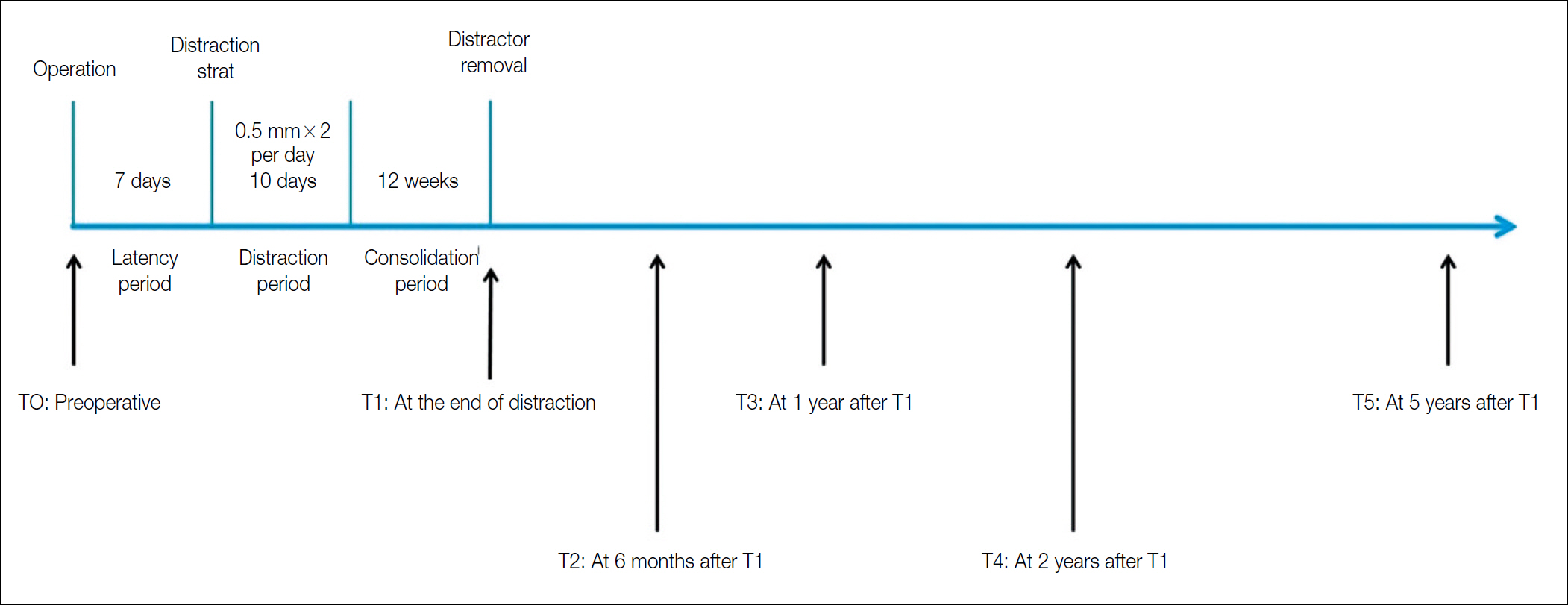
Fig. 2. Treatment protocol for maxillary distraction using an intraoral distractor.
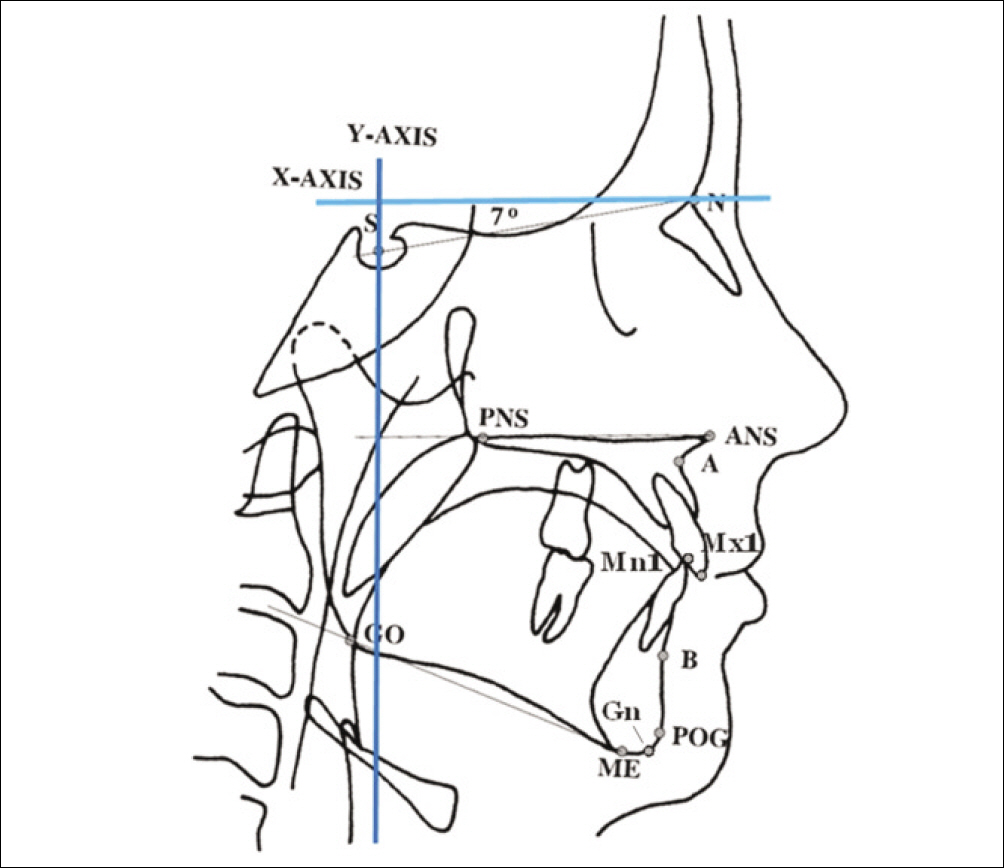
Fig. 3. Representation of landmarks and constructed lines used to identify craniofacial and dental parameters on lateral cephalometric radiograph. The following points were assessed; N: nasion, S: sella, ANS: anterior nasal spine, PNS: posterior nasal spine, A: subspinale, B: supramentale, Mx1: incisal edge of maxillary central incisor, Pg: pogonion, Gn: gnathion, Go: gonion, Me: menton, Mn1: incisal edge of mandibular central incisor, X-Axis: horizontal reference line-line through nasion rotated 7�upward from sella-nasion line, Y-Axis: vertical reference line-line perpendicular to horizontal reference line through sella.
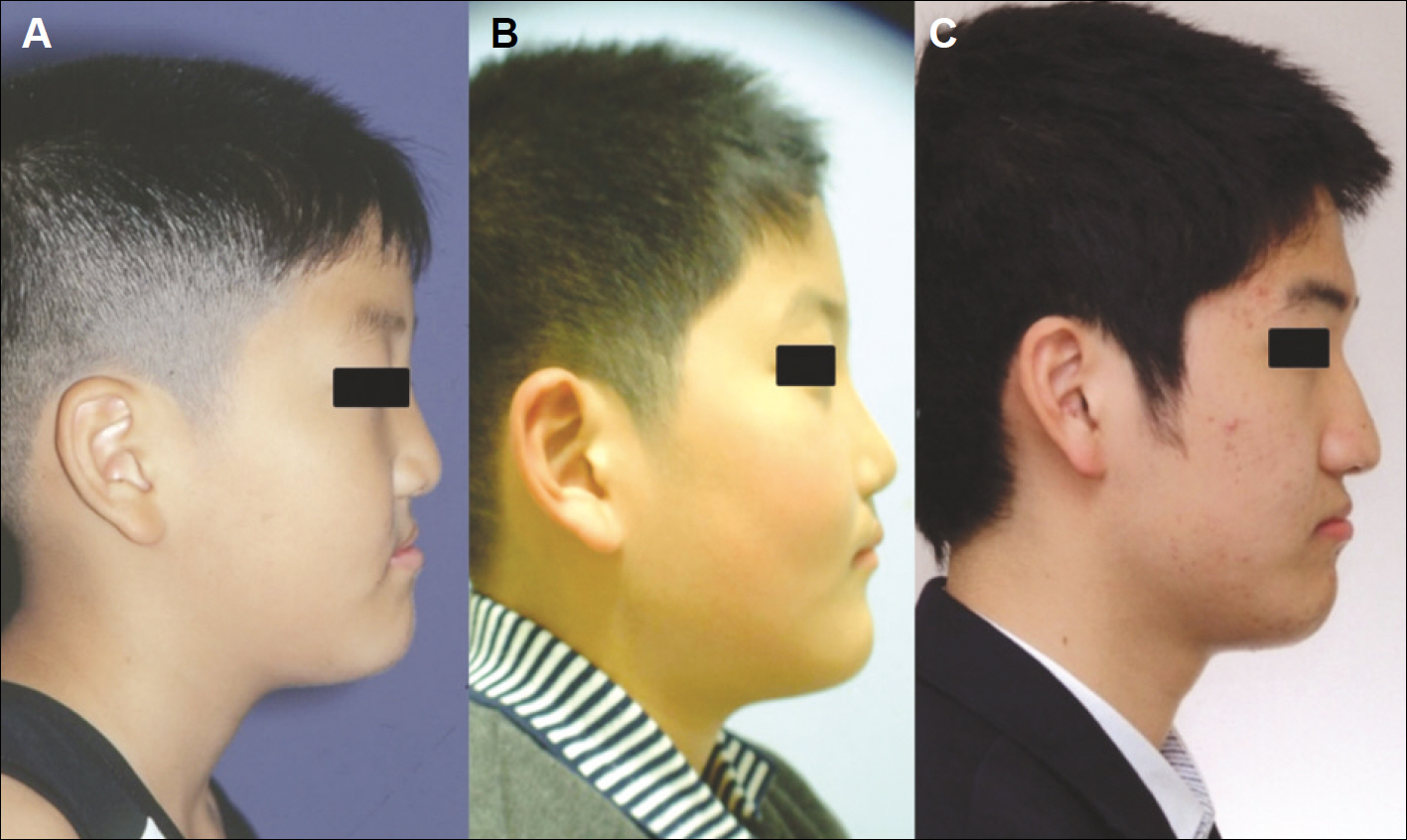
Fig. 4. Comparison of clinical photograph. A. Preoperative, B. After distraction osteogenesis, C. Post-op 5 years 8 months.

Fig. 5. Comparison of Lateral cephalogram. A. Preoperative, B. After distraction osteogenesis, C. Post-op 5 years 8 months.

Fig. 6. Comparison of Introral photograph, frontal view. A. Preoperative, B. after distraction osteogenesis.

Fig. 7. Superimposition of Lateral cephlogram.(T0-Black, T1-Red, T5-Green)
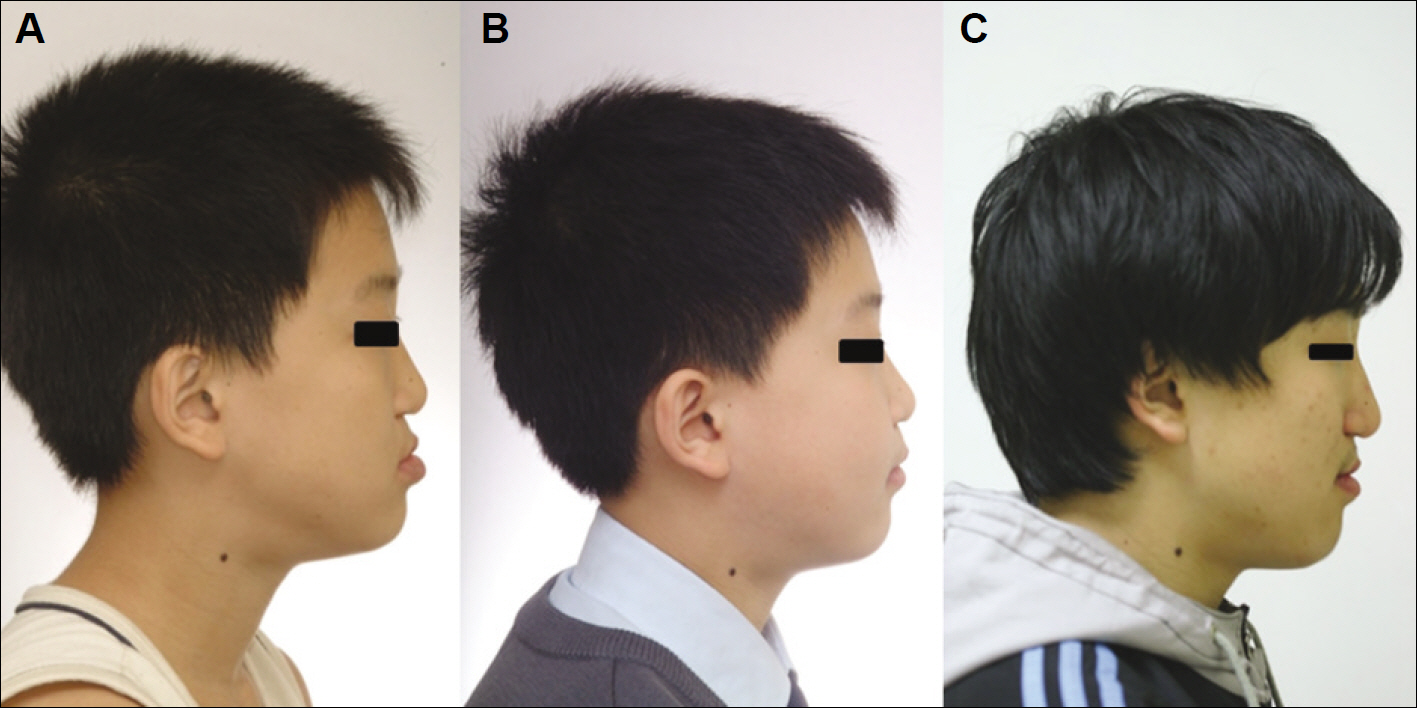
Fig. 8. Comparison of clinical photograph. A. Preoperative, B. After distraction osteogenesis, C. Post-op 5 years 3 months.

Fig. 9. Comparison of Lateral cephalogram. A. Preoperative, B. After distraction osteogenesis, C. Post-op 5 years 3 months.

Fig. 10. Superimposition of Lateral cephlogram.(T0-Black, T1-Red, T5-Green)
Reference
-
1. Rachmiel A, Aizenbud D, Peled M. Long-term results in maxillary deficiency using intraoral devices. Int J Oral Maxillofac Surg. 2005; 34:473–9.
Article2. Ross RB. Treatment variables affecting facial growth in complete unilateral cleft lip and palate. Cleft Palate J. 1987; 24:5–77.3. Erbe M, Stoelinga PJ, Leenen RJ. Long-term results of segmental repositioning maxilla in cleft palate patients without previously grafted alveolo-palatal cleft. J Craniomaxillofac Surg. 1996; 24:109–17.4. Posnick JC, Dagys AP. Skeletal stability and relapse patterns after Le Fort I maxillary osteotomy fixed with miniplates: the unilateral cleft lip and palate deformity. Plast Reconstr Surg. 1994; 94:924–32.5. McCarthy JG, Schreiber J, Karp N, Thorne CH, Grayson BH. Lengthening the human mandible by gradual distraction. Plast Reconstr Surg. 1992; 89:1–8.
Article6. Polley JW, Figueroa AA. Management of severe maxillary deficiency in childhood and adolescence through distraction osteogenesis with an external, adjustable, rigid distraction device. J Craniofac Surg. 1997; 8:181–5.
Article7. Madsen DP, Sampson WJ, Townsend GC. Craniofacial reference plane variation and natural head position. Eur J Orthod. 2008; 30:532–40.
Article8. Kanno T, Takahashi T, Takano H, Funaki K, Ichida T. Simultaneous maxilla-mandibular distraction osteogenesis using a subcutaneous device for a bilateral cleft lip and palate patient. Asian J Oral Maxillofac Surg. 2006; 18:303–8.9. Figueroa AA, Polley JW, Friede H, Ko EW. Long-term skeletal stability after maxillary advancement with distraction osteogenesis using a rigid external distraction device in cleft maxillary deformities. Plast Reconstr Surg. 2004; 114:1382–92.
Article10. Harada K, Sato M, Omura K. Maxillary distraction in patients with cleft deformity using a rigid external distraction device: a pilot study on the distraction ratio of the maxilla to the device. Scand J Plast Reconstr Surg Hand Surg. 2004; 38:277–80.
Article11. Yamauchi K, Mitsugi M, Takahashi T. Maxillary distraction osteogenesis using Le Fort I osteotomy without intraoperative down-fracture. Int J Oral Maxillofac Surg. 2006; 35:493–8.
Article12. Rachmiel A, Rozen N, Peled M, Lewinson D. Characterization of midface maxillary membranous bone formation during distraction osteogenesis. Plast Reconstr Surg. 2002; 109:1611–20.
Article13. Satoh K, Mitsukawa N, Tosa Y, Kadamatsu K, Hosaka Y. Simultaneous hybrid of maxillary Le Fort I halo distraction and mandibular set-back for patients with severe cleft jaw deformity. J Craniofac Surg. 2006; 17:962–9.
Article14. Proffit WR, Phillips C, Prewitt JW, Turvey TA. Stability after surgical orthodontic correction of skeletal Class III malocclusion. 2. Maxillary advancement. Int J Adult Orthodon Orthognath Surg. 1991; 6:71–80.15. Hoffman GR, Brennan PA. The skeletal stability of one-piece Le Fort 1 osteotomy to advance the maxilla; Part 1. Stability resulting from non-bone grafted rigid fixation. Br J Oral Maxillofac Surg. 2004; 42:221–5.16. Harada K, Sato M, Omura K. Long-term skeletal and dental changes in patients with cleft lip and palate after maxillary distraction: a report of three cases treated with a rigid external distraction device. Cranio. 2005; 23:152–7.
Article17. Cheung LK, Chua HD, Hägg MB. Cleft maxillary distraction versus orthognathic surgery: clinical morbidities and surgical relapse. Plast Reconstr Surg. 2006; 118:996–1008.
Article18. Cheung LK, Chua HD, Bendeus M. Distraction or osteotomy for the correction of maxillary cleft deformities: which is better? Ann R Australas Coll Dent Surg. 2004; 17:57–63.19. Thongdee P, Samman N. Stability of maxillary surgical movement in unilateral cleft lip and palate with preceding alveolar bone grafting. Cleft Palate Craniofac J. 2005; 42:664–74.
Article20. Louis PJ, Waite PD, Austin RB. Long-term skeletal stability after rigid fixation of Le Fort I osteotomies with advancements. Int J Oral Maxillofac Surg. 1993; 22:82–6.21. Wang XX, Wang X, Yi B, Li ZL, Liang C, Lin Y. Internal midface distraction in correction of severe maxillary hypoplasia secondary to cleft lip and palate. Plast Reconstr Surg. 2005; 116:51–60.
Article22. Cho BC, Kyung HM. Distraction osteogenesis of the hypoplastic midface using a rigid external distraction system: the results of a one to six-year followup. Plast Reconstr Surg. 2006; 118:1201–12.
Article23. Cheung LK, Chua HD. A meta-analysis of cleft maxillary osteotomy and distraction osteogenesis. Int J Oral Maxillofac Surg. 2006; 35:14–24.
Article24. Rachmiel A, Laufer D, Jackson IT, Lewinson D. Midface membranous bone lengthening: A one-year histological and morphological followup of distraction osteogenesis. Calcif Tissue Int. 1998; 62:370–6.
Article25. Kusnoto B, Figueroa AA, Polley JW. Radiographic evaluation of bone formation in the pterygoid region after maxillary distraction with a rigid external distraction (RED) device. J Craniofac Surg. 2001; 12:109–17.
Article26. Kanno T, Takahashi T, Ariyoshi W, Tsujisawa T, Haga M, Nishihara T. Tensile mechanical strain up-regulates Runx2 and osteogenic factor expression inhuman periosteal cells: implications for distraction osteogenesis. J Oral Maxillofac Surg. 2005; 63:499–504.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Distraction osteogenesis in patients with hemifacial microsomia
- Finite element analysis of anterior maxillary segmental distraction osteogenesis using asymmetric distractors in patients with unilateral cleft lip and palate
- Long-term follow-up of early cleft maxillary distraction
- Gradual distraction technique for maxillary protraction: Report of 2 Cases
- A study on the maxillary dental arch and palate of unilateral cleft lip and palate individuals
