A Case of Cholethorax Developed by Unknown Cause
- Affiliations
-
- 1Department of Internal Medicine, Chungbuk National University College of Medicine, Cheongju, Korea. kimlee@chungbuk.ac.kr
- 2Department of Thoracic and Cardiovascular Surgery, Chungbuk National University College of Medicine, Cheongju, Korea.
- KMID: 1442858
- DOI: http://doi.org/10.4046/trd.2011.70.3.261
Abstract
- Cholethorax is a bilious pleural effusion caused by a pleurobiliary fistula or leakage of bile into the pleural space. Most cases of cholethorax arise from a complication of abdominal trauma, hepatobiliary infection, or invasive procedures or surgery of hepatobiliary system. However, we experienced a case of a patient with cholethorax of unknown origin. There was no evidence of pleurobiliary fistula or leakage of bile from the hepatobiliary system although we examined the patient with various diagnostic tools including chest and abdominal computed tomography, endoscopic retrograde cholangiopancreatography, tubography, bronchofiberscopy, hepatobiliary scintigraphy and video-assisted thoracoscopic surgery. Herein we report a case of cholethorax for which the specific cause was not identified. The patient was improved by percutaneous drainage of pleural bile.
Keyword
MeSH Terms
Figure
-
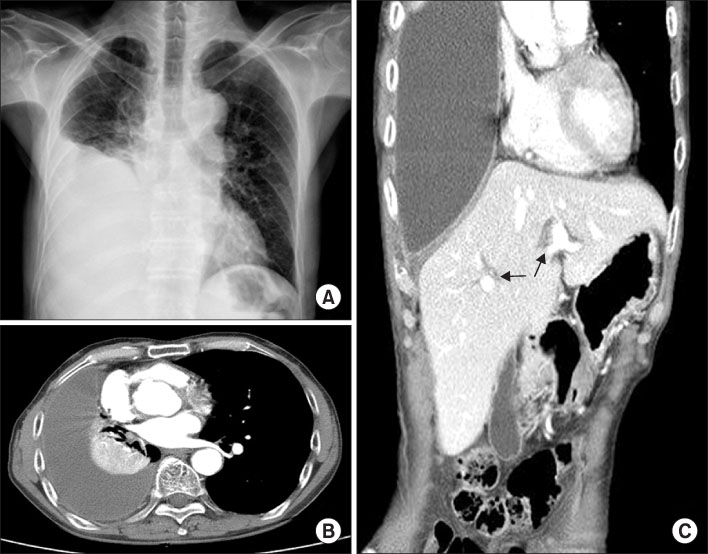
Figure 1 (A) Chest X-ray shows right pleural effusion. (B) Chest CT scan shows large amount of pleural effusion with passive atelectasis. (C) Abdomen CT scan shows mild intrahepatic duct dilatation (arrows). CT: computer tomography.

Figure 2 Percutaneously needle aspirated pleural effusion was dark greenish colored fluid.

Figure 3 (A) The retrograde cholangiopanrceatography shows no evidence of stricture, obstruction of biliary tree or leakage of contrast media. (B) Retrograde cholangiography shows no evidence of biliary tree abnormality or leakage of contrast media. (C) Contrast media injected into pleural cavity via Pigtail cathether. There is no evidence of fistula or leakage of contrast media into extrapleural space.
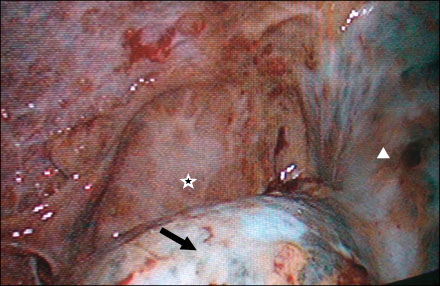
Figure 4 Video assisted thoracic surgery shows severe thickening of pleura with multiple adhesions. Star indicates right diaphragm and bile stained visceral pleura was seen at right upper lobe (triangle) and right lower lobe (arrow).
Reference
-
1. Amir-Jahed AK, Sadrieh M, Farpour A, Azar H, Namdaran F. Thoracobilia: a surgical complication of hepatic echinococcosis and amebiasis. Ann Thorac Surg. 1972. 14:198–205.2. Franklin DC, Mathai J. Biliary pleural fistula: a complication of hepatic trauma. J Trauma. 1980. 20:256–258.3. Strange C, Allen ML, Freedland PN, Cunningham J, Sahn SA. Biliopleural fistula as a complication of percutaneous biliary drainage: experimental evidence for pleural inflammation. Am Rev Respir Dis. 1988. 137:959–961.4. Ichikawa T, Yamada T, Takagi H, Abe T, Ito H, Sakurai S, et al. Transcatheter arterial embolization-induced bilious pleuritis in a patient with hepatocellular carcinoma. J Gastroenterol. 1997. 32:405–409.5. Oparah SS, Mandal AK. Traumatic thoracobiliary (pleurobiliary and bronchobiliary) fistulas: clinical and review study. J Trauma. 1978. 18:539–544.6. Light RW, Lee G. Textbook of pleural diseases. 2008. 2nd ed. London: Hodder Arnold.7. Lee SH, Lee KJ, Kim SY, Lee SK, Jung KS, Park BH, et al. Bilioptysis caused by bronchobiliary fistula secondary to sclerosing therapy of liver cyst. Tuberc Respir Dis. 2010. 69:119–123.8. Park CS, Lee SJ, Do GW, Oh SY, Cho H, Kim MS, et al. A case of cholethorax following percutaneous transhepatic cholangioscopy. Tuberc Respir Dis. 2008. 65:131–136.9. Feld R, Wechsler RJ, Bonn J. Biliary-pleural fistulas without biliary obstruction: percutaneous catheter management. AJR Am J Roentgenol. 1997. 169:381–383.10. Sheik-Gafoor MH, Singh B, Moodley J. Traumatic thoracobiliary fistula: report of a case successfully managed conservatively, with an overview of current diagnostic and therapeutic options. J Trauma. 1998. 45:819–821.11. Brunaud L, Sebbag H, Bresler L, Tortuyaux JM, Boissel P. Left hepatic duct injury and thoracobiliary fistula after abdominal blunt trauma. Hepatogastroenterology. 2000. 47:1227–1229.12. Rowe PH. Bilothorax--an unusual problem. J R Soc Med. 1989. 82:687–688.13. Pisani RJ, Zeller FA. Bilious pleural effusion following liver biopsy. Chest. 1990. 98:1535–1537.14. Córdoba López A, Monterrubio Villar J, Bueno Alvarez-Arenas I. Biliothorax unrelated to fistula: a rare complication in gallbladder disease. Arch Bronconeumol. 2008. 44:396–397.15. Sewell CM, Clarridge JE, Young EJ, Guthrie RK. Clinical significance of coagulase-negative staphylococci. J Clin Microbiol. 1982. 16:236–239.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Cholethorax following Percutaneous Transhepatic Cholangioscopy
- Aortic dissection presenting as fever of unknown origin
- A Case of Transfusion Induced Malaria Presenting as a Fever of Unknown Origin
- A Case of Acute Retroviral Syndrome Presenting as a Fever of Unknown Origin
- Clinical characteristics of children with mental retardation of unknown etiology in Korea
