Rotational pectoral musculocutaneous flap for the repair of gastric conduit necrosis in cervical esophagogastrostomy
- Affiliations
-
- 1Department of Thoracic and Cardiovascular Surgery, Seoul St. Mary's Hospital, Seoul, Korea. medkjj@hanmail.net
- 2Department of Thoracic and Cardiovascular Surgery, St. Paul's Hospital, The Catholic University of Korea College of Medicine, Seoul, Korea.
- KMID: 1437540
- DOI: http://doi.org/10.4174/jkss.2012.83.6.393
Abstract
- We experienced a case of wide necrosis of the cervical gastric conduit during esophageal cancer surgery. We attempted to repair this defect with various methods including conservative care, stents two times, and sternocleidomastoid muscle flap without successful results. Finally, we were able to reconstruct the gastric conduit defect with rotational pectoralis major musculocutaneous (PMM) flap. PMM flap is thought to be a reconstruction method applicable to the intractable gastric conduit defect.
MeSH Terms
Figure
-
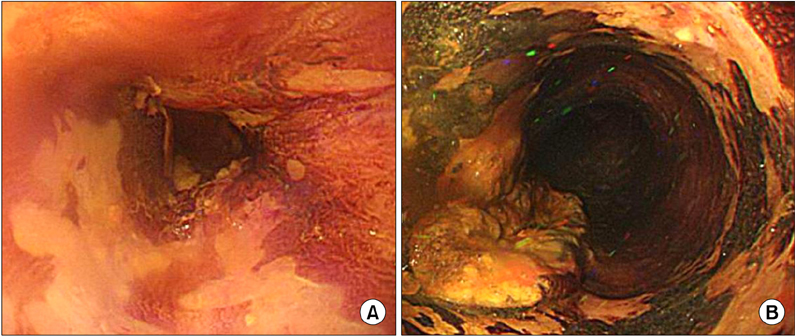
Fig. 1 Postchemotherapy esophagoscopy showed two masses from incisor 18 cm (A) and 30 cm (B). The pathology report showed that both lesions were squamous cell carcinoma.
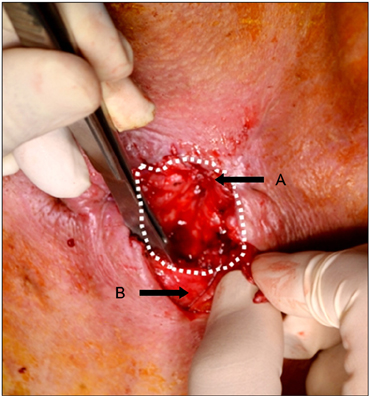
Fig. 2 Gastrocutaneous fistula. There was a 4 × 5 cm gastric conduit defect on anterior aspect (A, proximal esophagus; B, gastric conduit; dashed line, fistula extent).

Fig. 3 Reconstructive surgery using the musculocutaneous (PMM) flap. (A) The pectoralis major musculocutaneous flap was mobilized about 4 cm wide. And we made a subcutaneous tunnel up to the level of clavicle to connect the chest and defect site with caution to PMM flap vascular compression. (B) Closure of the defect of gastric conduit with rotating PMM flap by interrupted sutures with 4-0 vicryl sutures. (C) The wounds were completed with skin graft.

Fig. 4 Final postoperative esophagogram showed no leakage and passage disturbance (arrow, level of gastric conduit necrosis).
Reference
-
1. Motohiro H, Sumiko Y, Toshimasa T, Akiko N, Kazumasa F, Shoji N, et al. Pectoralis myocutaneous flap with T-tube drainage for cervical anastomotic leakage after salvage operation. Esophagus. 2006. 3:33–36.2. Turkyilmaz A, Eroglu A, Aydin Y, Tekinbas C, Muharrem Erol M, Karaoglanoglu N. The management of esophagogastric anastomotic leak after esophagectomy for esophageal carcinoma. Dis Esophagus. 2009. 22:119–126.3. Langer FB, Wenzl E, Prager G, Salat A, Miholic J, Mang T, et al. Management of postoperative esophageal leaks with the Polyflex self-expanding covered plastic stent. Ann Thorac Surg. 2005. 79:398–403.4. Lin CH, Lin CH, Wu CW, Liao CT. Sternocleidomastoid muscle flap: an option to seal off the esophageal leakage after free jejunal flap transfer: a case report. Chang Gung Med J. 2009. 32:224–229.5. Morita M, Ikeda K, Sugiyama M, Saeki H, Egashira A, Yoshinaga K, et al. Repair using the pectoralis major muscle flap for anastomotic leakage after esophageal reconstruction via the subcutaneous route. Surgery. 2010. 147:212–218.6. Shen KR, Austen WG Jr, Mathisen DJ. Use of a prefabricated pectoralis major muscle flap and pedicled jejunal interposition graft for salvage esophageal reconstruction after failed gastric pull-up and colon interposition. J Thorac Cardiovasc Surg. 2008. 135:1186–1187.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Man with Dysphagia after Cervical Esophagogastrostomy: A Case Report
- Survival of Musculocutaneous Flap with Draining Vein in Rats
- Considerations for Postoperative Results of Pressure Sores around Buttock Region by Musculocutaneous Flaps and Perforator Flaps
- Reconstruction of an abdominal wall defect using a latissimus dorsi musculocutaneous free flap after high-intensity focused ultrasound: a case report
- The reconstruction of soft tissue defects of cranioface using modified lower trapezius musculocutaneous flap
