Anterior Tibial Muscle Hernia Treated with Local Periosteal Rotational Flap: A Case Report
- Affiliations
-
- 1Department of Orthopedic Surgery, Bundang CHA Hospital, CHA University, Seongnam, Korea. orthopaedee@naver.com
- KMID: 1434076
- DOI: http://doi.org/10.12671/jkfs.2012.25.4.331
Abstract
- Tibialis anterior muscle hernia is the most common hernia among lower extremity muscles. This condition can be diagnosed by physical examination and radiologic findings, especially by dynamic ultrasonography. There are surgical methods of treatment for muscle hernia, including direct repair, fasciotomy, fascial patch grafting using autologous fascia lata or synthetic mesh. We report a case of tibialis anterior muscle hernia treated with local periosteal rotational flap. Because there are several advantages to the local periosteal rotational flap, such as lack of donor site morbidity, lack of skin irritation, low cost, simplicity, and an easy approach, this technique could be an option for tibialis anterior muscle hernia.
MeSH Terms
Figure
-

Fig. 1 The mass is prominent in a squatting position.
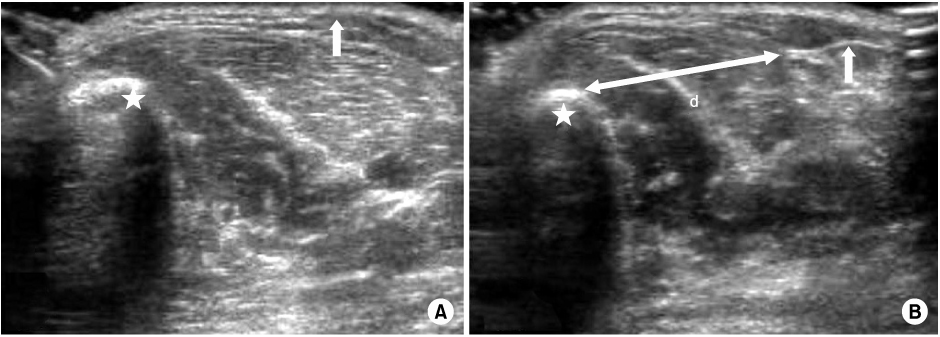
Fig. 2 Dynamic transverse ultrasonography of left anterolateral lower leg. (A) Image of ankle plantarflexion. Mild tibialis anterior herniation is seen between the tibia (star) and discontinued fascia (arrow). (B) Image of ankle dorsiflexion. The muscle hernia is prominent and the diameter (d) of the defect portion between the tibia (star) and fascia (arrow) is about 2.4 cm.

Fig. 3 Fascial defect is seen after skin and subcutaneous incision.
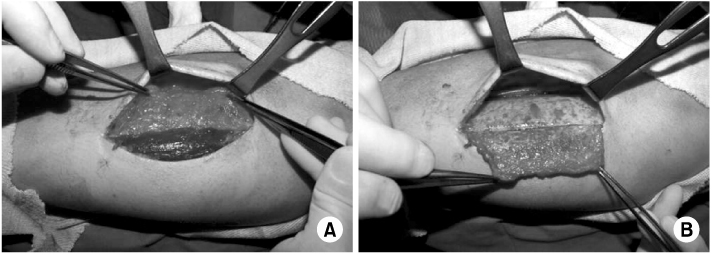
Fig. 4 (A) A periosteal flap is made to repair the fascial defect. (B) Turning the graft over the defective portion.
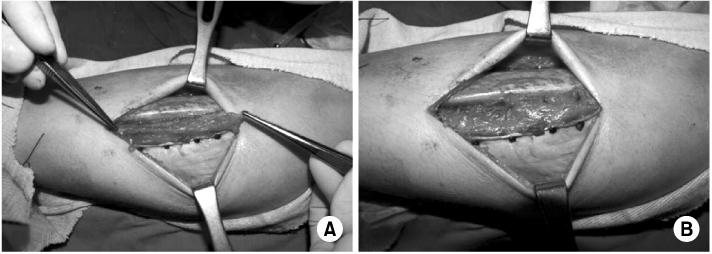
Fig. 5 (A) The graft is sufficient to cover the defect, but a partial graft is remained. (B) The remaining periosteal portion is overlapped and sutured for augmentation.
Reference
-
1. Bates DG. Dynamic ultrasound findings of bilateral anterior tibialis muscle herniation in a pediatric patient. Pediatr Radiol. 2001. 31:753–755.
Article2. Bloem JJ. The treatment of muscle hernias by fascial splitting. Br J Plast Surg. 1976. 29:291–294.
Article3. Chen CH, Chang CH, Su CI, et al. Arthroscopic single-bundle anterior cruciate ligament reconstruction with periosteum-enveloping hamstring tendon graft: clinical outcome at 2 to 7 years. Arthroscopy. 2010. 26:907–917.
Article4. Hølund T. Rupture and hernia of the tibials anterior muscle. J Bone Joint Surg Am. 1952. 24-A-3:678–679.5. Marić D, Madić D, Marić D, Stanković M, Smajić M. Anterior tibial muscle hernia-reconstruction with periosteal patch plasty. Vojnosanit Pregl. 2009. 66:1015–1018.
Article6. Marques A, Brenda E, Amarante MT. Bilateral multiple muscle hernias of the leg repaired with Marlex mesh. Br J Plast Surg. 1994. 47:444–446.
Article7. Miniaci A, Rorabeck CH. Compartment syndrome as a complication of repair of a hernia of the tibialis anterior. A case report. J Bone Joint Surg Am. 1986. 68:1444–1445.
Article8. Miniaci A, Rorabeck CH. Tibialis anterior muscle hernia: a rationale for treatment. Can J Surg. 1987. 30:79–80.9. Siliprandi L, Martini G, Chiarelli A, Mazzoleni F. Surgical repair of an anterior tibialis muscle hernia with Mersilene mesh. Plast Reconstr Surg. 1993. 91:154–157.
Article10. Wolfort GF, Mogelvang C, Filtzer HS. Anterior tibial compartment syndrome following muscle hernia repair. Arch Surg. 1973. 106:97–99.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Perforator Based Tibialis Anterior Segmental Muscle Island Flap in Lower Extremity Reconstruction
- An Experimental Study of Neochondrogenesis with Reversed Intraarticular Periosteal Flap in Rabbits
- Healing of the Bony Gap with Periosteal Osteogenesis After Tibial Diaphysectomy in Adult: Report of A Case
- Wide Cortical Drilling and Anterior-Based Periosteal Flap Reconstruction: Innovative Approach for Acquired Stenosis of External Auditory Canal
- Usefulness of the Keystone Flap in Lower Extremity Reconstruction in Patients with Anterior Tibial Artery Variation: A Case Report
