J Korean Soc Magn Reson Med.
2013 Mar;17(1):1-7. 10.13104/jksmrm.2013.17.1.1.
Transient Splenial Lesions in the Splenium of Corpus Callosum in Seven Patients: MR Findings and Clinical Correlations
- Affiliations
-
- 1Department of Radiology, Chungnam National University Hospital, Chungnam National University School of Medicine, Korea. leeinho1974@hanmail.net
- 2Department of Anesthesiology and Pain Medicine, Bestian Daejeon Hospital, Korea.
- KMID: 1426745
- DOI: http://doi.org/10.13104/jksmrm.2013.17.1.1
Abstract
- PURPOSE
The purpose of this study is to correlate the imaging findings and the clinical findings in patients with transient splenial lesions (TSL).
MATERIALS AND METHODS
Total of 7 patients (M: F = 4: 3; age range 11 - 38 years, mean age 25.5 years) were studied between November 2006 and April 2011. The MRI findings and clinical findings in all patients were retrospectively reviewed. The location, MR signal intensity, restricted diffusion, enhancement pattern and reversibility from the follow up images were reviewed. Clinical features were reviewed with respect to the presented symptoms, signs, treatment and outcome.
RESULTS
The lesions were located in the splenium of corpus callosum in all patients. All lesions showed high signal intensity on diffusion weighted imaging (DWI), and six patients showed restricted diffusion on the apparent diffusion coefficient (ADC) map. ADC map was not available in one patient. All lesions (n = 7) showed high signal intensity on the T2 weighted image (T2WI). Five of the patients (71.4%) with follow up images (range 7 - 34 days) showed complete resolution of focal high signal intensity on DWI, with recovery of ADC values as well as T2WI. After contrast media administration, none of the lesions showed any enhancements. All lesions with various etiologies including TB medication were developed in younger age patients and showed reversibility after the acceptable period of minimum 7 days with conservative treatment.
CONCLUSION
All TSL showed nonspecific imaging findings, including restricted diffusion on DWI and ADC map on the initial images. However, reversibility of the lesions and the young age preference can be a characteristic finding of TSL with acceptable period of minimum 7 days. In addition, to keep it in mind that various etiologies including TB medication may cause TSL, is important for radiologists as well as clinicians.
Keyword
MeSH Terms
Figure
-
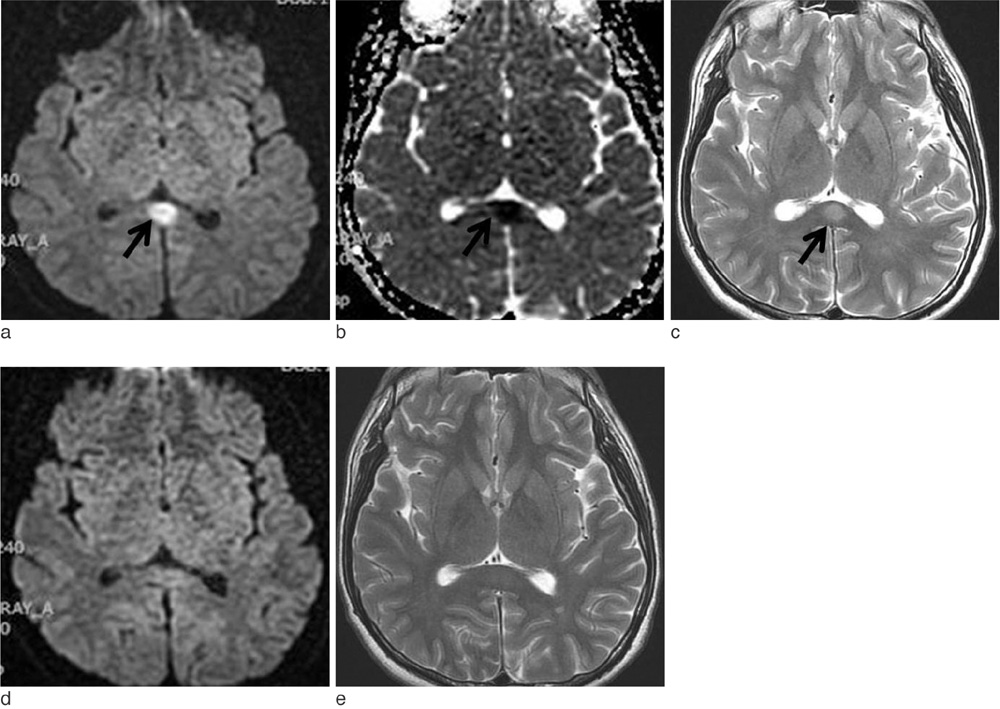
Fig. 1 A 19-year-old man presented with headaches and dizziness (patient #4). a, b. DWI and ADC map show restricted diffusion on the splenium (arrows). c. T2WI shows high signal intensity on the splenium (arrow). d, e. Follow up DWI and T2WI show complete resolution on the splenium (arrows) obtained 14 days after those of (a) and (c).
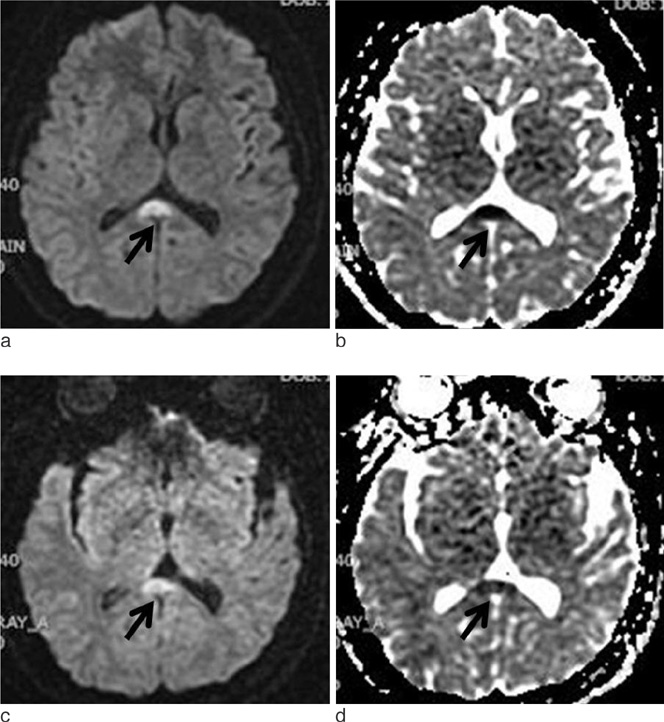
Fig. 2 A 30-year-old woman presented with headache (patient #3). a, b. DWI and ADC map show restricted diffusion on the splenium (arrows). c, d. Follow up DWI and ADC map show partial resolution on the splenium (arrows), obtained 5 days after those of (a) and (b).
Reference
-
1. Takanashi J, Barkovich AJ, Yamaguchi K, Kohno Y. Influenza-associated encephalitis/encephalopathy with a reversible lesion in the splenium of the corpus callosum: a case report and literature review. AJNR Am J Neuroradiol. 2004; 25:798–802.2. Takanashi J, Barkovich AJ, Shiihara T, et al. Widening spectrum of a reversible splenial lesion with transiently reduced diffusion. AJNR Am J Neuroradiol. 2006; 27:836–838.3. Kim SS, Chang KH, Kim ST, et al. Focal lesion in the splenium of the corpus callosum in epileptic patients: antiepileptic drug toxicity? AJNR Am J Neuroradiol. 1999; 20:125–129.4. Maeda M, Shiroyama T, Tsukahara H, Shimono T, Aoki S, Takeda K. Transient splenial lesion of the corpus callosum associated with antiepileptic drugs: evaluation by diffusion-weighted MR imaging. Eur Radiol. 2003; 13:1902–1906.5. Polster T, Hoppe M, Ebner A. Transient lesion in the splenium of the corpus callosum: three further cases in epileptic patients and a pathophysiological hypothesis. J Neurol Neurosurg Psychiatry. 2001; 70:459–463.6. Oster J, Doherty C, Grant PE, Simon M, Cole AJ. Diffusion-weighted imaging abnormalities in the splenium after seizures. Epilepsia. 2003; 44:852–854.7. Mirsattari SM, Lee DH, Jones MW, Blume WT. Transient lesion in the splenium of the corpus callosum in an epileptic patient. Neurology. 2003; 60:1838–1841.8. Honda K, Nishimiya J, Sato H, et al. Transient splenial lesion of the corpus callosum after acute withdrawal of antiepileptic drug: a case report. Magn Reson Med Sci. 2006; 5:211–215.9. Bulakbasi N, Kocaoglu M, Tayfun C, Ucoz T. Transient splenial lesion of the corpus callosum in clinically mild influenza-associated encephalitis/encephalopathy. AJNR Am J Neuroradiol. 2006; 27:1983–1986.10. Tada H, Takanashi J, Barkovich AJ, et al. Clinically mild encephalitis/encephalopathy with a reversible splenial lesion. Neurology. 2004; 63:1854–1858.11. Gallucci M, Limbucci N, Paonessa A, Caranci F. Reversible focal splenial lesions. Neuroradiology. 2007; 49:541–544.12. Hagemann G, Mentzel HJ, Weisser H, Kunze A, Terborg C. Multiple reversible MR signal changes caused by Epstein-Barr virus encephalitis. AJNR Am J Neuroradiol. 2006; 27:1447–1449.13. Takanashi J, Miyamoto T, Ando N, et al. Clinical and radiological features of rotavirus cerebellitis. AJNR Am J Neuroradiol. 2010; 31:1591–1595.14. Oztoprak I, Engin A, Gumus C, Egilmez H, Oztoprak B. Transient splenial lesions of the corpus callosum in different stages of evolution. Clin Radiol. 2007; 62:907–913.15. Kobata R, Tsukahara H, Nakai A, et al. Transient MR signal changes in the splenium of the corpus callosum in rotavirus encephalopathy: value of diffusion-weighted imaging. J Comput Assist Tomogr. 2002; 26:825–828.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Transient Isolated Splenial Lesion of the Corpus Callosum After New Onset Seizure
- Transient Splenial Lesion of the Corpus Callosum in Patients with Infectious Disease
- Transient splenial lesions of the corpus callosum and infectious diseases
- Reversible Splenial Lesion in the Corpus Callosum on MRI after Ingestion of a Herbicide Containing Glufosinate Ammonium: A Case Report
- Reversible Lesion in The splenium of The Corpus Callosum Induced by Topiramate in a Patient with Migraine
