Clin Orthop Surg.
2013 Mar;5(1):49-54. 10.4055/cios.2013.5.1.49.
MRI Measurement of Neuroforaminal Dimension at the Index and Supradjacent Levels after Anterior Lumbar Interbody Fusion: A Prospective Study
- Affiliations
-
- 1Twin Cities Spine Center, Minneapolis, MN, USA. woojinchomd@aol.com
- 2Department of Radiology, Abbott Northwestern Hospital, Minneapolis, MN, USA.
- KMID: 1402326
- DOI: http://doi.org/10.4055/cios.2013.5.1.49
Abstract
- BACKGROUND
Anterior interbody fusion has previously been demonstrated to increase neuroforaminal height in a cadaveric model using cages. No prior study has prospectively assessed the relative change in magnetic resonance imaging (MRI) demonstrated neuroforaminal dimensions at the index and supradjacent levels, after anterior interbody fusion with a corticocancellous allograft in a series of patients without posterior decompression. The objective of this study was to determine how much foraminal dimension can be increased with indirect foraminal decompression alone via anterior interbody fusion, and to determine the effect of anterior lumbar interbody fusion on the dimensions of the supradjacent neuroforamina.
METHODS
A prospective study comparing pre- and postoperative neuroforaminal dimensions on MRI scan among 26 consecutive patients undergoing anterior lumbar interbody fusion without posterior decompression was performed. We studies 26 consecutive patients (50 index levels) that had undergone anterior interbody fusion followed by posterior pedicle screw fixation without distraction or foraminotomy. We used preoperative and postoperative MRI imaging to assess the foraminal dimensions at each operated level on which the lumbar spine had been operated. The relative indirect foraminal decompression achieved was calculated. The foraminal dimension of the 26 supradjacent untreated levels was measured pre- and postoperatively to serve as a control and to determine any effects after anterior interbody fusion.
RESULTS
In this study, 8 patients underwent 1 level fusion (L5-S1), 12 patients had 2 levels (L4-S1) and 6 patients had 3 levels (L3-S1). The average increase in foraminal dimension was 43.3% (p < 0.05)-19.2% for L3-4, 57.1% for L4-5, and 40.1% for L5-S1. Mean pre- and postoperative supradjacent neuroforaminal dimension measurements were 125.84 mm2 and 124.89 mm2, respectively. No significant difference was noted (p > 0.05).
CONCLUSIONS
Anterior interbody fusion with a coriticocancellous allograft can significantly increase neuroforaminal dimension even in the absence of formal posterior distraction or foraminotomy; anterior interbody fusion with a coriticocancellous allograft has little effect on supradjacent neuroforaminal dimensions.
Keyword
MeSH Terms
Figure
-
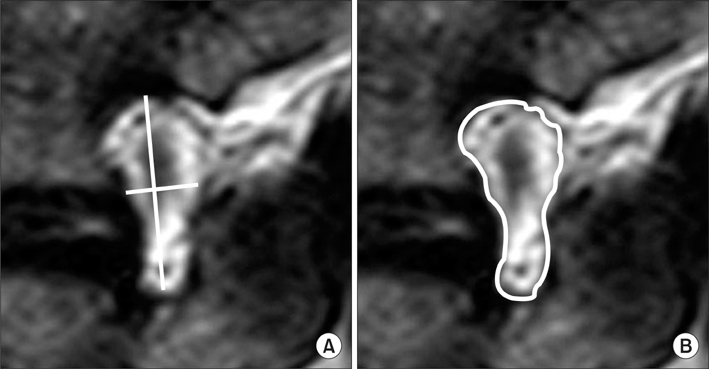
Fig. 1 Methods for measuring foraminal dimension; manual measurement (A), software measurement (B).

Fig. 2 Measurement of index foraminal dimensions in preoperative (A) and postoperative (B) magnetic resonance imaging.

Fig. 3 Measurement of supradjacent foraminal dimensions on preoperative (A) and postoperative (B) magnetic resonance imaging.
Reference
-
1. Sekerci Z, Ugur A, Ergun R, Sanli M. Early changes in the cervical foraminal area after anterior interbody fusion with polyetheretherketone (PEEK) cage containing synthetic bone particulate: a prospective study of 20 cases. Neurol Res. 2006. 28(5):568–571.2. Bartels RH, Donk R, van Azn RD. Height of cervical foramina after anterior discectomy and implantation of a carbon fiber cage. J Neurosurg. 2001. 95:1 Suppl. 40–42.3. Shen FH, Samartzis D, Khanna N, Goldberg EJ, An HS. Comparison of clinical and radiographic outcome in instrumented anterior cervical discectomy and fusion with or without direct uncovertebral joint decompression. Spine J. 2004. 4(6):629–635.4. Jenis LG, An HS, Gordin R. Foraminal stenosis of the lumbar spine: a review of 65 surgical cases. Am J Orthop (Belle Mead NJ). 2001. 30(3):205–211.5. Infusa A, An HS, Glover JM, McGrady L, Lim TH, Riley LH 3rd. The ideal amount of lumbar foraminal distraction for pedicle screw instrumentation. Spine (Phila Pa 1976). 1996. 21(19):2218–2223.6. Humke T, Grob D, Grauer W, Sandler A, Dvorak J. Foraminal changes with distraction and compression of the L4/5 and L5/S1 segments. Eur Spine J. 1996. 5(3):183–186.7. Sandhu HS, Turner S, Kabo JM, et al. Distractive properties of a threaded interbody fusion device: an in vivo model. Spine (Phila Pa 1976). 1996. 21(10):1201–1210.8. Chen D, Fay LA, Lok J, Yuan P, Edwards WT, Yuan HA. Increasing neuroforaminal volume by anterior interbody distraction in degenerative lumbar spine. Spine (Phila Pa 1976). 1995. 20(1):74–79.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anterior Interbody Fusion using a Horizontal Cylinder Cage in a Degenerative Lumbar Spine
- Height Changes of Intervertebral Disc and Neural Foramen after Anterior Lumbar Interbody Fusion in the Lumbar Spine
- Effect of the Pedicle Screw Fixation on the Anterior Lumbar Interbody Fusion Using the Freeze - Dried Structural Allograft
- The Changes of the Dimension of Intervertebral Disc,-Neural Foramen and Spinal Canal after Anterior Lumbar Interbody Fusion in the Lumbar Spine
- Anterior Lumbar Interbody Fusion Using BAK Cage for Treatment of Failed Back Surgery Syndrome
