Mucin-Producing Carcinoma of the Gallbladder: Evaluation by Magnetic Resonance Cholangiopancreatography in Three Cases
- Affiliations
-
- 1Hepatobiliary and Pancreatic Surgery Division, National Cancer Center Hospital, Tokyo 104-0045, Japan.
- 2Diagnostic Radiology Division, National Cancer Center Hospital, Tokyo 104-0045, Japan. honaya@ncc.go.jp
- 3Pathology Division, National Cancer Center Hospital, Tokyo 104-0045, Japan.
- KMID: 1392944
- DOI: http://doi.org/10.3348/kjr.2012.13.5.637
Abstract
- We report three cases of mucin-producing carcinoma of the gallbladder, along with the magnetic resonance (MR) findings, especially the findings on a MR cholangiopancreatography. In our cases, linear or curvilinear streaks were detected running along the long axis of an enlarged gallbladder (mucus thread sign). When such findings were seen, a mucin-producing carcinoma of the gallbladder should be included as a differential diagnosis. Thus, gadolinium-enhanced MR imaging is mandatory for the precise diagnosis of the mucin-producing carcinoma of the gallbladder.
Keyword
MeSH Terms
Figure
-
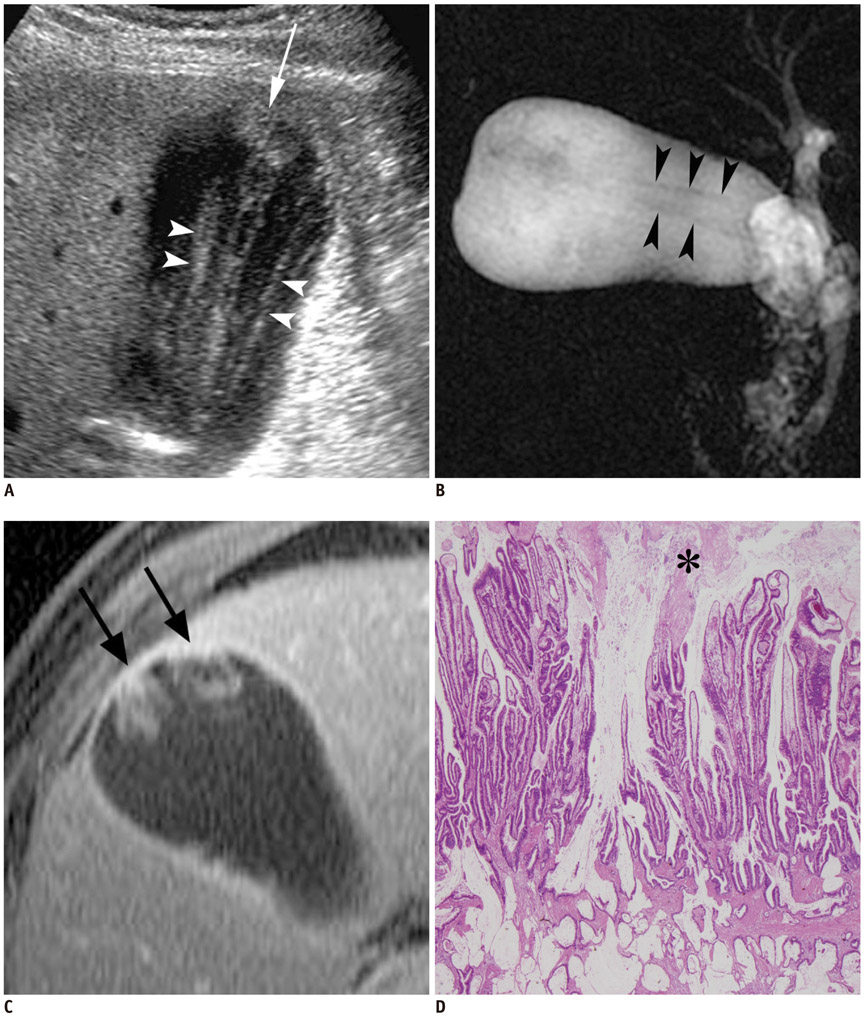
Fig. 1 Intracystic papillary adenocarcinoma in 59-year-old man. A. Right intercostal Ultrasonography performed with 5.0 MHz probe demonstrates that tumors in fundus (arrow) and several striations of variable width (arrowheads) are almost same echogenicity. B. Thick-slab magnetic resonance cholangiopancreatography (repetition time msec/echo time msec, infinite/1023 [effective]; 60-mm-thick slab) depicts some fine hypointense striations (arrowheads) in moderately enlarged gallbladder showing marked hyperintensity. C. Axial T1-weighted fat-saturated gradient-recalled echo (175/2.1; flip angle, 70°) obtained 3 min after Gd-DTPA injection reveals well-enhanced papillary projections (arrows) in fundus that could be clearly differentiated from mucus striations. D. Microscopically, significant mucin (asterisk) sticks to surface of papillary carcinoma, and floating in mucin are clumps or strands of epithelium, some of which contain malignant cells (Hematoxylin & Eosin staining; original magnification × 200).

Fig. 2 Papillary adenocarcinoma invading subserosal layer with lymph node metastasis in 53-year-old woman. A. Coronal thin-section magnetic resonance cholangiopancreatography (MRCP) (infinite/99.6 [effective], 4-mm-thick sections) clearly shows some striations running along long axis (arrowheads) of gallbladder. B. Coronal gadolinium-enhanced T1-weighted image (150/1.8; flip angle, 70°) anterior to (A) demonstrates protruding lesion (arrow) in body of enlarged gallbladder. C. Subcostal ultrasonography performed with 9.0 MHz probe reveals hyperechoic polypoid lesion with papillary surface (arrows) that seems to produce threading striations (arrowheads) similar to those visualized on MRCP images.
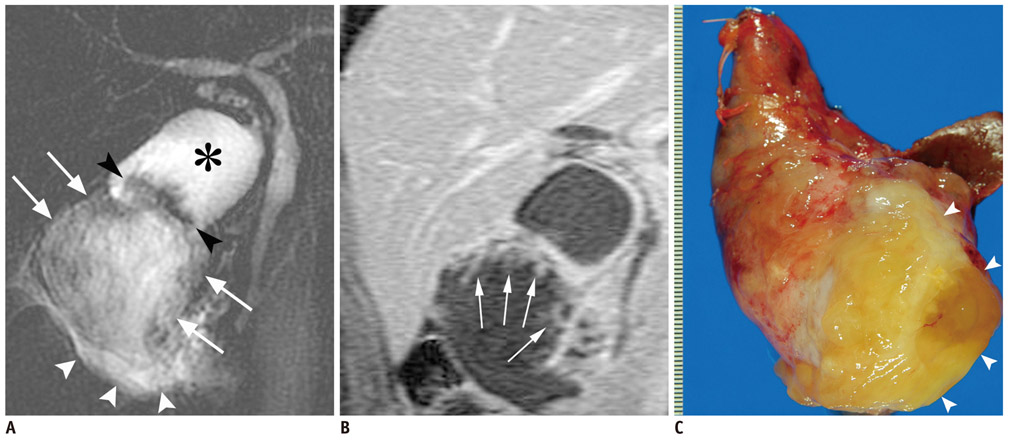
Fig. 3 Mucinous carcinoma with peritoneal dissemination in 48-year-old woman. A. Thick-slab magnetic resonance cholangiopancreatography (infinite/1023 [effective], 60-mm-thick slab) shows two separate compartments of gallbladder. Markedly hyperintense portion near cystic duct (asterisk) corresponds to native lumen of gallbladder, while weakly hyperintense fundic part (arrows) filled with mucus materials shows hypointense streaks of mucinous carcinoma extending to highly thickened wall. Separation between two parts is seen as localized wall thickening with papillary surface observed as luminal lesion in fundus (black arrowheads). Poorly formed area of hyperintensity surrounds gallbladder (white arrowheads), which is indicative of pooled mucin due to perforation. B. Coronal gadolinium-enhanced T1-weighted image (150/1.8; flip angle, 70°) shows several papillary enhancements with irregularly thickening wall (arrows). C. Macroscopically, fundus of enlarged gallbladder was covered thickly with overflowing gelatinous mucin (arrowheads).
Reference
-
1. Levy AD, Murakata LA, Rohrmann CA Jr. Gallbladder carcinoma: radiologic-pathologic correlation. Radiographics. 2001. 21:295–314. questionnaire 549-555.2. Lim JH, Yi CA, Lim HK, Lee WJ, Lee SJ, Kim SH. Radiological spectrum of intraductal papillary tumors of the bile ducts. Korean J Radiol. 2002. 3:57–63.3. Ishibashi H, Hachisuka K, Yamaguchi A, Isogai M, Fukada S, Kato S, et al. Mucin-producing gallbladder carcinoma: report of a case. Tan to Sui. 1986. 7:1173–1178.4. Tian H, Matsumoto S, Takaki H, Kiyosue H, Komatsu E, Okino Y, et al. Mucin-producing carcinoma of the gallbladder: imaging demonstration in four cases. J Comput Assist Tomogr. 2003. 27:150–154.5. Ozeki Y, Matsubara N, Saiga T, Homma M, Koyama A, Ichikawa T, et al. Mucus-producing cancer of the gallbladder: report of a case. Gastroenterol Endosc. 1991. 33:2439–2444.6. Huang CP, Chiou YY, Chou YH, Chiang JH, Chang CY. Imaging findings in mucin-producing carcinoma of the gallbladder. J Formos Med Assoc. 2006. 105:427–430.7. Lim JH, Yoon KH, Kim SH, Kim HY, Lim HK, Song SY, et al. Intraductal papillary mucinous tumor of the bile ducts. Radiographics. 2004. 24:53–66. discussion 66-67.8. Miyazaki T, Yamashita Y, Tsuchigame T, Yamamoto H, Urata J, Takahashi M. MR cholangiopancreatography using HASTE (half-Fourier acquisition single-shot turbo spin-echo) sequences. AJR Am J Roentgenol. 1996. 166:1297–1303.9. Irie H, Honda H, Tajima T, Kuroiwa T, Yoshimitsu K, Makisumi K, et al. Optimal MR cholangiopancreatographic sequence and its clinical application. Radiology. 1998. 206:379–387.10. Nobusawa H, Hashimoto T, Munechika H, Soejima K, Seino N, Kurashita Y, et al. [US and CT findings of mucinous carcinomas of the gallbladder]. Nihon Igaku Hoshasen Gakkai Zasshi. 1994. 54:1359–1367.11. Miyake H, Hori Y, Dono S, Mori H. Low attenuation intratumoral matrix: CT and pathologic correlation. J Comput Assist Tomogr. 2000. 24:761–772.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Incidentally detected gallbladder agenesis in a child: the importance of identifying anatomic structure
- Radiologic Evaluation and Differential Diagnosis of Gallbladder Cancer
- Synchronous Undifferentiated Carcinoma of Gallbladder in a Patient with Intrahepatic Intraductal Papillary Mucinous Neoplasia (b-IPMN)
- Clinical Significance of Anomalous Pancreaticobiliary Ductal Union Diagnosed by Endoscopic Retrograde Cholangiopancreatography
- Alpha-Fetoprotein-Producing Carcinoma of the Gallbladder
