Histologic Characteristics of Hepatocellular Carcinomas Showing Atypical Enhancement Patterns on 4-Phase MDCT Examination
- Affiliations
-
- 1Department of Radiology, Research Institute of Radiological Science, Yonsei University College of Medicine, Seoul 120-752, Korea. kimnex@yuhs.ac
- KMID: 1392937
- DOI: http://doi.org/10.3348/kjr.2012.13.5.586
Abstract
OBJECTIVE
To retrospectively define which histologic characteristics of small-sized hepatocellular carcinomas (HCCs) are related to atypical dynamic enhancement on multi-detector computed tomography (MDCT) imaging.
MATERIALS AND METHODS
Seventy-three patients with 83 HCCs (3 cm or less in diameter) were included in this study. All patients underwent 4-phase MDCT imaging and subsequent surgery within eight weeks. Two independent radiologists blinded to the histologic findings retrospectively classified the HCCs as either typical (showing increased enhancement on arterial phase images followed by washout in late phase images) or atypical lesions demonstrating any other enhancement pattern. From the original pathologic reports, various histologic characteristics including gross morphology, nuclear histologic grades, presence of capsule formation, and capsule infiltration when a capsule was present, were compared among the two groups.
RESULTS
An atypical enhancement pattern was seen in 30 (36.2%) of the 83 HCCs. The mean size of atypical HCCs (1.71 +/- 0.764) was significantly smaller than that of typical HCCs (2.31 +/- 0.598, p < 0.001). Atypical HCCs were frequently found to be vaguely nodular in gross morphology (n = 13, 43.3%) and to have grade I nuclear grades (n = 17, 56.7%). Capsule formation was significantly more common in typical HCCs (p < 0.001). Capsular infiltration was also more common in typical HCCs (p = 0.001).
CONCLUSION
HCCs showing atypical dynamic enhancement on MDCT imaging are usually smaller than typical HCCs, vaguely nodular type in gross morphology in most cases, and well-differentiated in nuclear grades, and they lack of capsule formation or capsular infiltration.
Keyword
MeSH Terms
-
Adult
Carcinoma, Hepatocellular/pathology/*radiography/surgery
Chi-Square Distribution
Contrast Media/diagnostic use
Diagnosis, Differential
Female
Humans
Image Enhancement
Iohexol/analogs & derivatives/diagnostic use
Liver Neoplasms/pathology/*radiography/surgery
Male
Middle Aged
Radiographic Image Interpretation, Computer-Assisted
Retrospective Studies
Tomography, X-Ray Computed/*methods
Figure
-

Fig. 1 43-year-old man with underlying B-viral hepatitis. (A) Precontrast, (B) hepatic arterial, (C) portal venous, (D) equilibrium phase images from 4-phase multi-detector CT scan. Hypoattenuating lesion (arrow) is seen on precontrast phase image (A). Lesion (arrow) shows increased arterial enhancement on arterial phase image (B) and washout of contrast enhancement on portal venous (C) and equilibrium phase images (D). (E) Gross specimen of lesion (arrow). Histologic examination demonstrated poorly differentiated (nuclear grade III) hepatocellular carcinoma of expanding type gross morphology with partial capsule formation and infiltration.
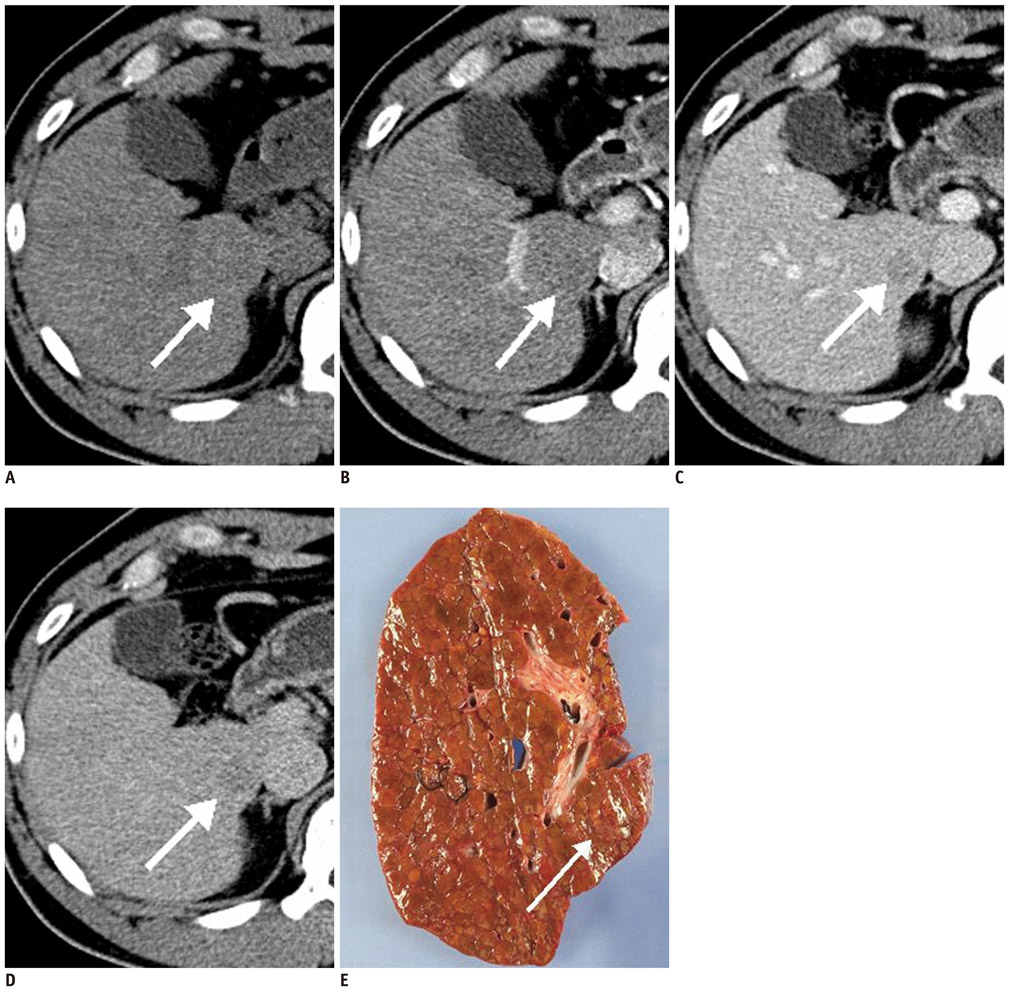
Fig. 2 49-year-old man with B-viral liver cirrhosis. (A) Precontrast, (B) hepatic arterial, (C) portal venous, (D) equilibrium phase images from 4-phase multi-detector CT scan. On precontrast (A) and arterial phase (B), lesion (arrow) showed isoattenuation compared to surrounding parenchyma. On portal venous (C) and equilibrium phase (D), lesion (arrow) shows hypoattenuation compared to surrounding parenchyma. (E) Gross specimen of lesion (arrow). Histologic examination showed well-differentiated (nuclear grade I) hepatocellular carcinoma of vaguely nodular type in gross morphology without capsule formation.
Reference
-
1. Choi BI, Lee JM. Advancement in HCC imaging: diagnosis, staging and treatment efficacy assessments: imaging diagnosis and staging of hepatocellular carcinoma. J Hepatobiliary Pancreat Sci. 2010. 17:369–373.2. Bruix J, Sherman M. American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma: an update. Hepatology. 2011. 53:1020–1022.3. Colli A, Fraquelli M, Casazza G, Massironi S, Colucci A, Conte D, et al. Accuracy of ultrasonography, spiral CT, magnetic resonance, and alpha-fetoprotein in diagnosing hepatocellular carcinoma: a systematic review. Am J Gastroenterol. 2006. 101:513–523.4. Willatt JM, Hussain HK, Adusumilli S, Marrero JA. MR Imaging of hepatocellular carcinoma in the cirrhotic liver: challenges and controversies. Radiology. 2008. 247:311–330.5. Marrero JA, Hussain HK, Nghiem HV, Umar R, Fontana RJ, Lok AS. Improving the prediction of hepatocellular carcinoma in cirrhotic patients with an arterially-enhancing liver mass. Liver Transpl. 2005. 11:281–289.6. Parkin DM, Bray F, Ferlay J, Pisani P. Estimating the world cancer burden: Globocan 2000. Int J Cancer. 2001. 94:153–156.7. Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, Bozzetti F, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996. 334:693–699.8. Bolondi L, Gaiani S, Celli N, Golfieri R, Grigioni WF, Leoni S, et al. Characterization of small nodules in cirrhosis by assessment of vascularity: the problem of hypovascular hepatocellular carcinoma. Hepatology. 2005. 42:27–34.9. Takayama T, Makuuchi M, Hirohashi S, Sakamoto M, Okazaki N, Takayasu K, et al. Malignant transformation of adenomatous hyperplasia to hepatocellular carcinoma. Lancet. 1990. 336:1150–1153.10. Edmondson HA, Steiner PE. Primary carcinoma of the liver: a study of 100 cases among 48,900 necropsies. Cancer. 1954. 7:462–503.11. Forner A, Vilana R, Ayuso C, Bianchi L, Solé M, Ayuso JR, et al. Diagnosis of hepatic nodules 20 mm or smaller in cirrhosis: Prospective validation of the noninvasive diagnostic criteria for hepatocellular carcinoma. Hepatology. 2008. 47:97–104.12. Hwang SH, Yu JS, Kim KW, Kim JH, Chung JJ. Small hypervascular enhancing lesions on arterial phase images of multiphase dynamic computed tomography in cirrhotic liver: fate and implications. J Comput Assist Tomogr. 2008. 32:39–45.13. Lee J, Lee WJ, Lim HK, Lim JH, Choi N, Park MH, et al. Early hepatocellular carcinoma: three-phase helical CT features of 16 patients. Korean J Radiol. 2008. 9:325–332.14. Shimizu A, Ito K, Koike S, Fujita T, Shimizu K, Matsunaga N. Cirrhosis or chronic hepatitis: evaluation of small (<or=2-cm) early-enhancing hepatic lesions with serial contrast-enhanced dynamic MR imaging. Radiology. 2003. 226:550–555.15. Hytiroglou P, Park YN, Krinsky G, Theise ND. Hepatic precancerous lesions and small hepatocellular carcinoma. Gastroenterol Clin North Am. 2007. 36:867–887. vii16. Monzawa S, Ichikawa T, Nakajima H, Kitanaka Y, Omata K, Araki T. Dynamic CT for detecting small hepatocellular carcinoma: usefulness of delayed phase imaging. AJR Am J Roentgenol. 2007. 188:147–153.17. Monzawa S, Omata K, Shimazu N, Yagawa A, Hosoda K, Araki T. Well-differentiated hepatocellular carcinoma: findings of US, CT, and MR imaging. Abdom Imaging. 1999. 24:392–397.18. Nakashima Y, Nakashima O, Hsia CC, Kojiro M, Tabor E. Vascularization of small hepatocellular carcinomas: correlation with differentiation. Liver. 1999. 19:12–18.19. Yoon SH, Lee JM, So YH, Hong SH, Kim SJ, Han JK, et al. Multiphasic MDCT enhancement pattern of hepatocellular carcinoma smaller than 3 cm in diameter: tumor size and cellular differentiation. AJR Am J Roentgenol. 2009. 193:W482–W489.20. Kim SH, Lee WJ, Lim HK, Park CK. SPIO-enhanced MRI findings of well-differentiated hepatocellular carcinomas: correlation with MDCT findings. Korean J Radiol. 2009. 10:112–120.21. International Consensus Group for Hepatocellular Neoplasia. Pathologic diagnosis of early hepatocellular carcinoma: a report of the international consensus group for hepatocellular neoplasia. Hepatology. 2009. 49:658–664.22. Ishizaki M, Ashida K, Higashi T, Nakatsukasa H, Kaneyoshi T, Fujiwara K, et al. The formation of capsule and septum in human hepatocellular carcinoma. Virchows Arch. 2001. 438:574–580.23. Okuda K, Musha H, Nakajima Y, Kubo Y, Shimokawa Y, Nagasaki Y, et al. Clinicopathologic features of encapsulated hepatocellular carcinoma: a study of 26 cases. Cancer. 1977. 40:1240–1245.24. Nagao T, Inoue S, Goto S, Mizuta T, Omori Y, Kawano N, et al. Hepatic resection for hepatocellular carcinoma. Clinical features and long-term prognosis. Ann Surg. 1987. 205:33–40.25. Lai EC, Ng IO, Ng MM, Lok AS, Tam PC, Fan ST, et al. Long-term results of resection for large hepatocellular carcinoma: a multivariate analysis of clinicopathological features. Hepatology. 1990. 11:815–818.26. Ng IO, Lai EC, Ng MM, Fan ST. Tumor encapsulation in hepatocellular carcinoma. A pathologic study of 189 cases. Cancer. 1992. 70:45–49.27. Takayasu K, Muramatsu Y, Mizuguchi Y, Okusaka T, Shimada K, Takayama T, et al. CT Evaluation of the progression of hypoattenuating nodular lesions in virus-related chronic liver disease. AJR Am J Roentgenol. 2006. 187:454–463.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Dynamic MR Imaging of Hepatic Hemangioma and Hepatocellular: Findings and Differential Diagnosis
- A Comprehensive Review of Hepatocellular Carcinoma Enhancement Patterns in MRI: Emphasis on Gadoxetate-Enhanced Imaging
- Focal Hepatic Lesions: Dynamic Multi-slice MR Imaging
- Nodular Hepatocellular Carcinoma: Contrast Enhancement Patterns on Three-Phase Spiral CT
- Comparison of Ferucarbotran-Enhanced MRI and Triple-Phase MDCT for the Detection of Hepatocellular Carcinoma in Advanced Liver Cirrhosis
